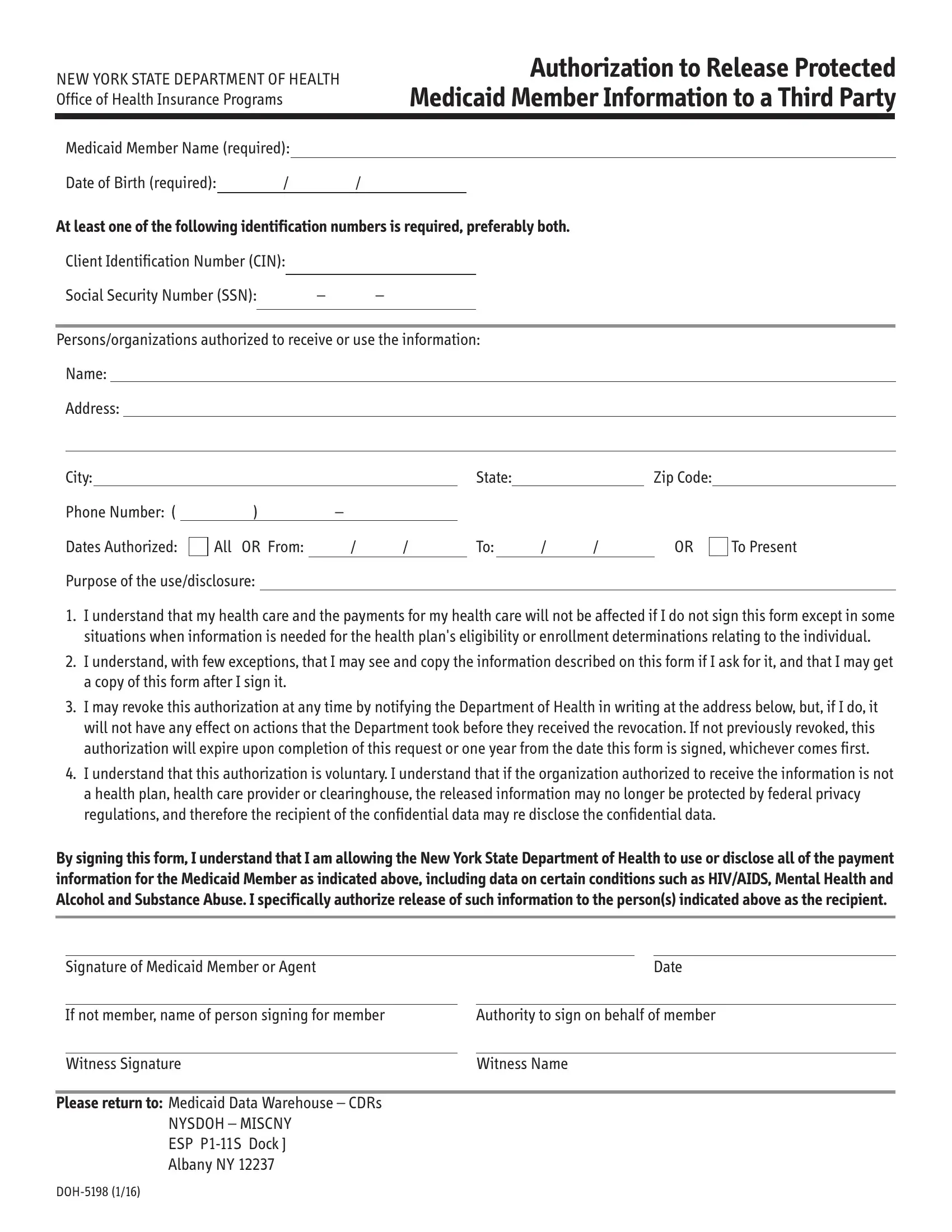
In navigating the complexities of healthcare information privacy and access, the DOH 5198 form stands out as a critical document within the New York State Department of Health's arsenal. It serves a pivotal role by granting authorization to release protected Medicaid member information to third parties. This form requires detailed information about the Medicaid member, including name, date of birth, and identification numbers such as the Client Identification Number (CIN) and Social Security Number (SSN), to ensure the accuracy and security of the data exchange. Additionally, it clearly outlines the scope of information release, specifying the persons or organizations authorized to receive the data, the duration of the authorization, and the purposes for which the information may be used or disclosed. An understanding of the conditions under which a Medicaid member may, or may not, revoke this authorization, and the implications of such revocation, is crucial for both members and third parties involved. Moreover, the form highlights the voluntary nature of this authorization and warns of potential privacy risks if the information is shared with entities outside the healthcare system. By signing the DOH 5198 form, Medicaid members actively participate in managing their healthcare information, navigating the delicate balance between privacy and the need for sharing critical health data.
| Question | Answer |
|---|---|
| Form Name | Form Doh 5198 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | authorization to release protected medicaid member information to a third party, p1, ssn, nysdoh 5198 form |
NEW YORK STATE DEPARTMENT OF HEALTH Office of Health Insurance Programs
Authorization to Release Protected Medicaid Member Information to a Third Party
Medicaid Member Name (required):
Date of Birth (required): |
/ |
/ |
At least one of the following identification numbers is required, preferably both.
Client Identification Number (CIN):
Social Security Number (SSN): |
– |
– |
|
|
|
|
|
|
|
|
|
Persons/organizations authorized to receive or use the information:
Name:
Address:
City: |
|
|
|
|
|
State: |
|
|
Zip Code: |
|
||
Phone Number: ( |
) |
– |
|
|
|
|
|
|
|
|
|
|
Dates Authorized: |
All OR From: |
/ |
/ |
|
To: |
|
/ |
/ |
|
OR |
To Present |
|
Purpose of the use/disclosure:
1.I understand that my health care and the payments for my health care will not be affected if I do not sign this form except in some situations when information is needed for the health plan's eligibility or enrollment determinations relating to the individual.
2.I understand, with few exceptions, that I may see and copy the information described on this form if I ask for it, and that I may get a copy of this form after I sign it.
3.I may revoke this authorization at any time by notifying the Department of Health in writing at the address below, but, if I do, it will not have any effect on actions that the Department took before they received the revocation. If not previously revoked, this authorization will expire upon completion of this request or one year from the date this form is signed, whichever comes first.
4.I understand that this authorization is voluntary. I understand that if the organization authorized to receive the information is not a health plan, health care provider or clearinghouse, the released information may no longer be protected by federal privacy regulations, and therefore the recipient of the confidential data may re disclose the confidential data.
By signing this form, I understand that I am allowing the New York State Department of Health to use or disclose all of the payment information for the Medicaid Member as indicated above, including data on certain conditions such as HIV/AIDS, Mental Health and Alcohol and Substance Abuse. I specifically authorize release of such information to the person(s) indicated above as the recipient.
Signature of Medicaid Member or Agent |
Date |
||
|
|
|
|
|
If not member, name of person signing for member |
Authority to sign on behalf of member |
|
|
|
|
|
|
Witness Signature |
Witness Name |
|
|
|
||
Please return to: Medicaid Data Warehouse – CDRs |
|
||
|
NYSDOH – MISCNY |
|
|
|
ESP |
|
|
|
Albany NY 12237 |
|
|