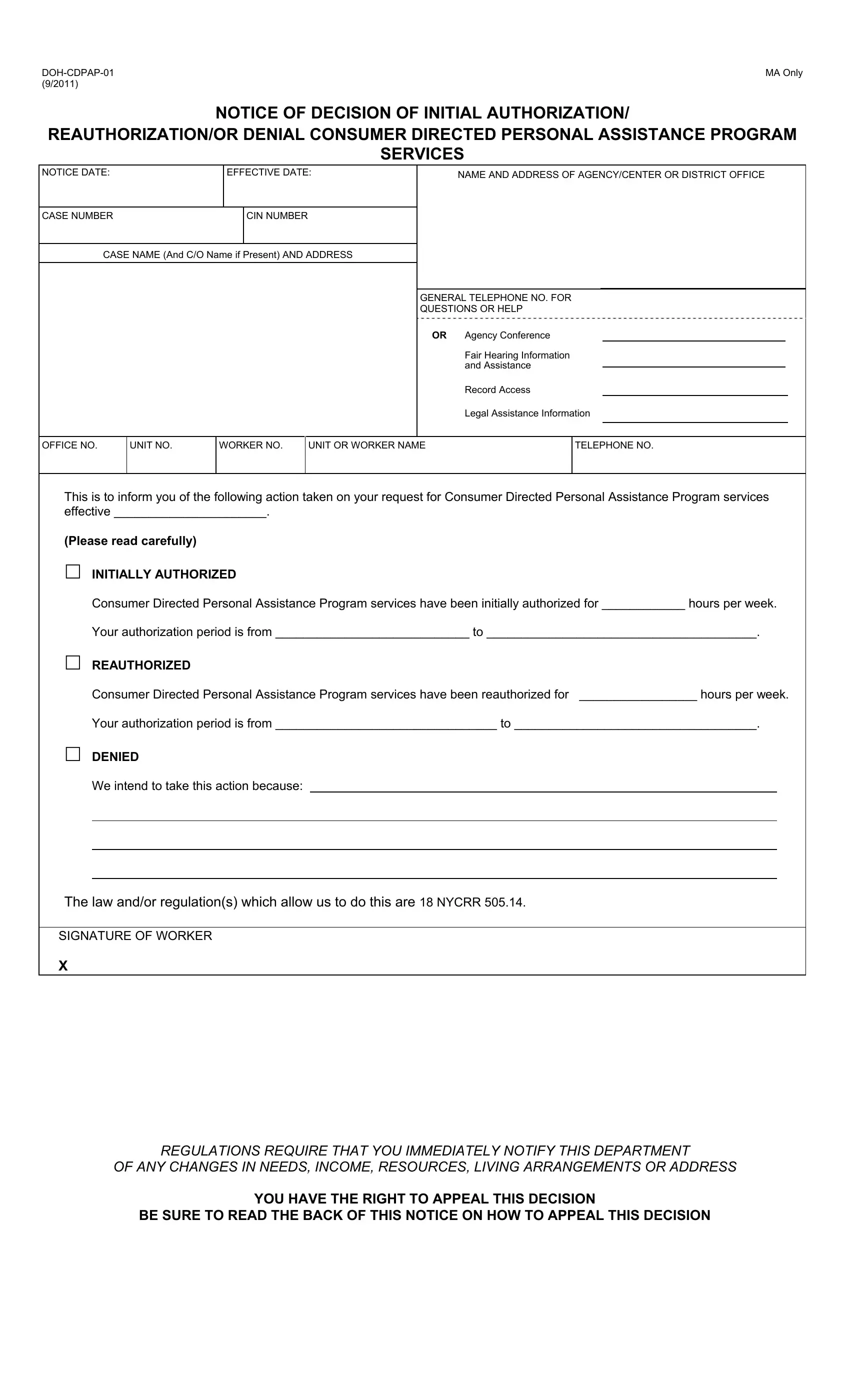
The DOH-CDPAP-01 form is a critical document within the New York State Department of Health's Consumer Directed Personal Assistance Program (CDPAP), offering individuals the power to manage their own health care services. This form serves as a notification tool, detailing decisions regarding initial authorizations, reauthorizations, or denials of CDPAP services. It outlines the specific duration and quantity of authorized services, providing clear instructions for the recipient regarding their rights and next steps. Essential information such as case and contact details, reasons for the decision based on specific regulations, and instructions for requesting a fair hearing or conference are included. This document emphasizes the importance of timely communication by the consumer concerning changes in their needs or circumstances and provides a gateway to legal aid for those in need. Furthermore, it underscores the availability of access to one’s file and documents, vital for preparing for appeals or understanding the decision made. The form is a testament to the structured yet consumer-focused approach of the CDPAP, ensuring that individuals are well-informed of their rights and the procedures to follow should they disagree with a decision made regarding their care.
| Question | Answer |
|---|---|
| Form Name | Form Doh Cdpap 01 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CIN, 2011, nys doh notice of decision for cdpap doh cdpap 02, nys doh notice of decision for cdpap doh cdpap 01 |
