Form Dol Lm 101 is a document that all businesses in the state of Maine must complete. The form is used to collect important information about the business, including its structure, officers, and contact information. Completing Form Dol Lm 101 is a necessary step in registering your business with the state of Maine. As such, it's important to understand what information is required on the form and how to complete it correctly. In this blog post, we'll take a closer look at Form Dol Lm 101 and provide tips for completing it accurately. Stay tuned!
| Question | Answer |
|---|---|
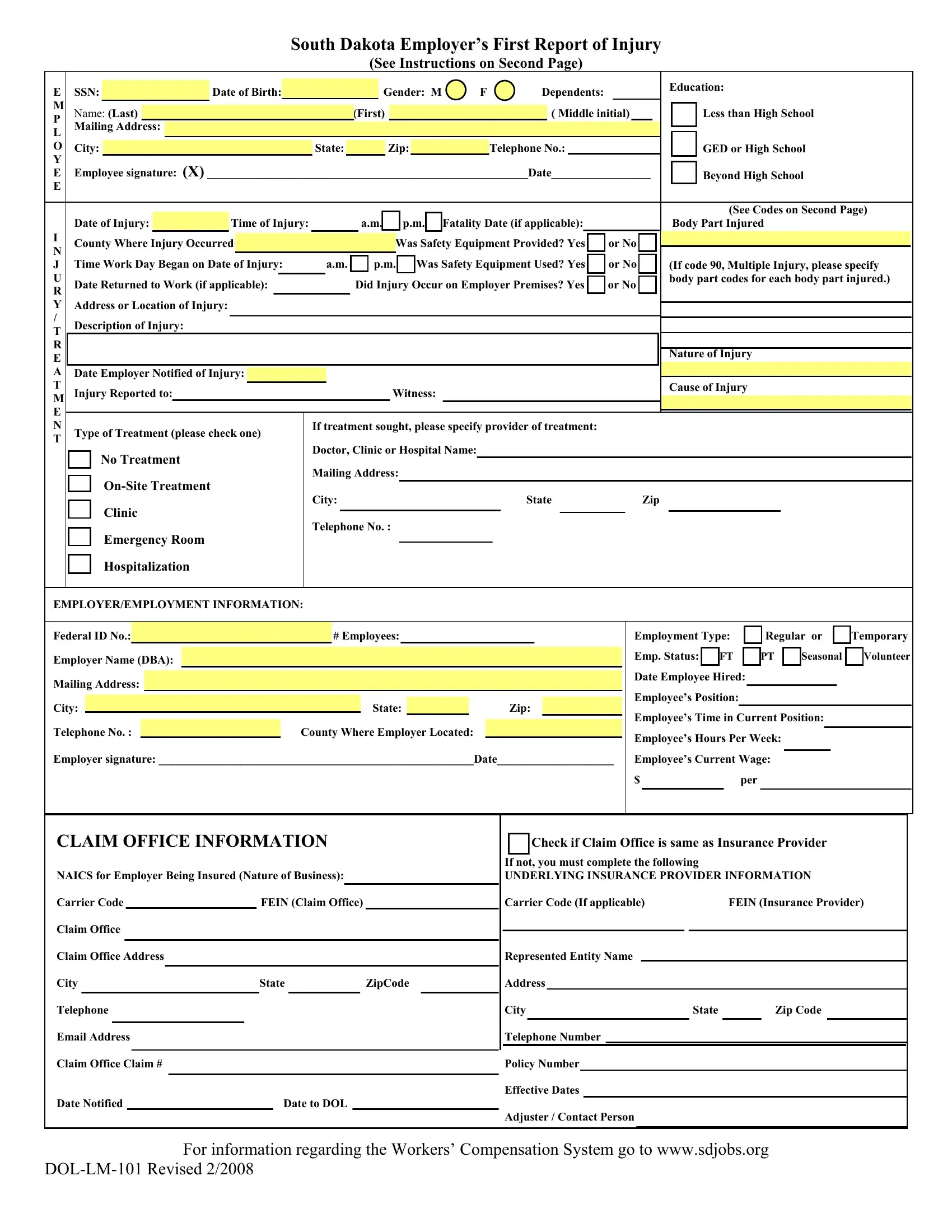
| Form Name | Form Dol Lm 101 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 1830, DBA, South_Dakota, Xerxes |

|
|
South Dakota Employer’s First Report of Injury |
|
|||
|
|
|
(See Instructions on Second Page) |
|
||
E |
SSN: |
Date of Birth: |
Gender: M |
F |
Dependents: |
Education: |
|
||||||
M |
Name: (Last) |
|
(First) |
|
( Middle initial) |
Less than High School |
P |
|
|
||||
L |
Mailing Address: |
|
|
|
|
|
O |
City: |
State: |
Zip: |
|
Telephone No.: |
GED or High School |
Y |
|
|
|
|
|
|
E |
Employee signature: (X) _______________________________________________________Date_________________ |
Beyond High School |
||||
E |
|
|
|
|
|
|
|
Date of Injury: |
|
Time of Injury: |
|
|
|
a.m. |
|
|
|
p.m. |
|
Fatality Date (if applicable): |
|
|
|
|
(See Codes on Second Page) |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Body Part Injured |
||||||||||
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
County Where Injury Occurred: |
|
|
|
|
|
|
|
|
|
Was Safety Equipment Provided? Yes |
|
or No |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Time Work Day Began on Date of Injury: |
|
a.m. |
|
|
p.m. |
|
|
Was Safety Equipment Used? Yes |
|
or No |
|
|
|
||||||||||
J |
|
|
|
|
|
|
|
|
(If code 90, Multiple Injury, please specify |
||||||||||||||
U |
|
|
|
|
|
|
|
|
|
|
|
body part codes for each body part injured.) |
|||||||||||
Date Returned to Work (if applicable): |
|
|
Did Injury Occur on Employer Premises? Yes |
|
or No |
|
|
||||||||||||||||
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YAddress or Location of Injury:
/ |
Description of Injury: |
|
|
|
|
|
|
|
|
||
T |
|
|
|
|
|
|
|
||||
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nature of Injury |
||
E |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
A |
Date Employer Notified of Injury: |
|
|
|
|
|
|
|
|
||
T |
Injury Reported to: |
|
|
|
|
|
Witness: |
|
|
Cause of Injury |
|
M |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
Type of Treatment (please check one) |
If treatment sought, please specify provider of treatment: |
|
|
|||||||
T |
|
|
|
|
|
|
|
||||
Doctor, Clinic or Hospital Name:
No Treatment
Mailing Address:
City:StateZip
Clinic
Telephone No. :
Emergency Room
Hospitalization
EMPLOYER/EMPLOYMENT INFORMATION:
Federal ID No.: |
|
|
|
|
|
|
|
# Employees: |
|
|
|
|
|
Employment Type: |
|
Regular or |
|
|
|
Temporary |
||||||||||||||
Employer Name (DBA): |
|
|
|
|
|
|
|
|
|
|
|
Emp. Status: |
|
|
|
|
PT |
|
Seasonal |
|
|
Volunteer |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
FT |
|
|
|
|
||||||||||||||||||
Mailing Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Date Employee Hired: |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee’s Position: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
City: |
|
|
|
|
|
|
|
|
|
State: |
|
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee’s Time in Current Position: |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Telephone No. : |
|
|
|
|
|
County Where Employer Located: |
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
Employee’s Hours Per Week: |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Employer signature: ______________________________________________________Date____________________ |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
Employee’s Current Wage: |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
per |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLAIM OFFICE INFORMATION |
|
|
|
|
|
Check if Claim Office is same as Insurance Provider |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If not, you must complete the following |
|
|
|
|||||||||||
NAICS for Employer Being Insured (Nature of Business): |
|
|
|
|
UNDERLYING INSURANCE PROVIDER INFORMATION |
||||||||||||||||||||||||||||
Carrier Code |
|
|
FEIN (Claim Office) |
|
|
|
Carrier Code (If applicable) |
|
|
|
FEIN (Insurance Provider) |
||||||||||||||||||||||
Claim Office |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Claim Office Address |
|
|
|
|
|
|
|
|
|
|
Represented Entity Name |
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
ZipCode |
Address |
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone |
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
Zip Code |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Email Address |
|
|
|
|
|
|
|
|
|
|
Telephone Number |
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Claim Office Claim # |
|
|
|
|
|
|
|
|
|
|
Policy Number |
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Effective Dates |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Date Notified |
|
|
Date to DOL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adjuster / Contact Person |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
For information regarding the Workers’ Compensation System go to www.sdjobs.org
GENERAL INSTRUCTIONS
EMPLOYEE
1.Notify employer immediately of injury, as required by SDCL
2.Complete all questions in the EMPLOYEE and INJURY/TREATMENT sections.
3.Sign the form.
4.Submit this form to your employer within three (3) business days after the injury.
EMPLOYER
1.Complete all questions in the EMPLOYER/EMPLOYMENT sections.
2.Sign the form.
3.Submit this form to your workers’ compensation insurance carrier within seven (7) days of knowledge of the occurrence of the injury, as required by SDCL
4.Give a copy of the form to the injured employee.
5.Keep the copy of the First Report of Injury for at least four (4) years from the date of injury, as required by SDCL
INSURER
1.Complete all questions in the CLAIM OFFICE INFORMATION sections at the bottom of the page.
2.Submit this form within ten (10) days of its receipt, as required by SDCL
SOUTH DAKOTA DEPARTMENT OF LABOR DIVISION OF LABOR AND MANAGEMENT 700 Governors Drive
Pierre SD
BODY PART CODES
02 |
Blindness one eye |
44 |
Chest, including ribs sternum, soft ribs |
78 |
Ring finger at metacarpal bone |
03 |
Blindness both eyes |
48 |
Internal |
79 |
Ring finger at proximal joint |
04 |
Deafness both ears |
49 |
Heart |
80 |
Ring finger at middle joint |
05 |
Deafness one ear |
51 |
Hip |
81 |
Ring finger at distal joint |
10 |
Multiple head injury |
52 |
Upper leg |
82 |
Little finger at metacarpal bone |
11 |
Skull |
53 |
Knee |
83 |
Little finger at proximal joint |
12 |
Brain |
54 |
Lower leg |
84 |
Little finger at middle joint |
13 |
Ear(s) |
55 |
Ankle |
85 |
Little finger at distal joint |
14 |
Eye(s) |
56 |
Foot |
86 |
Great toe metatarsal bone |
17 |
Mouth |
57 |
Toe (other than greater) |
87 |
Great toe at proximal joint |
19 |
Face (facial bones) |
58 |
Toe (greater) |
88 |
Great toe at distal joint |
20 |
Multiple neck injury |
60 |
Lungs |
90 |
Multiple injury |
21 |
Vertebrae |
61 |
Groin |
92 |
Other toe metatarsal bone |
22 |
Disc |
67 |
Thumb metacarpal bone |
93 |
Other toe at proximal joint |
24 |
Other |
68 |
Thumb at proximal joint |
94 |
Other toe at middle joint |
31 |
Upper arm |
69 |
Thumb at distal joint |
95 |
Other toe at distal joint |
32 |
Elbow |
70 |
Index finger at metacarpal bone |
96 |
Little toe metatarsal bone |
33 |
Lower |
71 |
Index finger at proximal joint |
97 |
Little toe at distal joint |
34 |
Wrist |
72 |
Index finger at middle joint |
|
|
35 |
Hand |
73 |
Index finger at distal joint |
|
|
37 |
Thumb |
74 |
Middle finger at metacarpal bone |
|
|
38 |
Shoulder |
75 |
Middle finger at proximal joint |
|
|
41 |
Upper Back |
76 |
Middle finger at middle joint |
|
|
42 |
Lower Back |
77 |
Middle finger at distal joint |
|
|
Cause of Injury Codes |
|
|
|
Nature of injury codes |
||
01 |
Body reaction/over reaction |
70 |
Striking against or stepping on |
|
|
|
|
(includes chemicals) |
|
|
|
00 |
Not applicable |
|
|
|
|
|
01 |
Allergy |
03 |
Temperature extremes |
78 |
Struck or injured by moving parts of machine |
|
02 |
Disfigurement |
13 |
Caught in/under/between |
81 |
Struck or injured, includes knife or sharp object, |
|
71 |
Occupational disease |
|
|
|
kicked, bit, etc. – struck by object, worker, |
|
72 |
Hearing loss |
|
|
|
patient, etc. |
|
|
|
25 |
Fall from elevation |
89 |
Hostile |
|
|
|
29 |
Fall from same level |
90 |
Other than physical cause of injury |
|
|
|
50 |
Motor vehicle |
94 |
Repetitive motion – callous, blister, etc. |
|
|
|
56 |
Bending/Lifting |
97 |
Repetitive |
|
|
|
65 |
Machinery/Equipment |
99 |
Other |
|
|
|