The Department of Public Health (DPH) form 4192 is a Certificate of Need (CON) application. A CON is a required process by the state of Illinois in order to ensure that all new and proposed healthcare services, facilities, and equipment are necessary, cost-effective, and meet the needs of the population. The DPH form 4192 must be completed and submitted to the DPH before any construction or renovation can take place. In this blog post, we will discuss what is included on the DPH form 4192 and how to complete it. We will also provide examples of completed forms so that you can better understand what is required. Stay tuned for our next post, which will discuss submission requirements and timelines.
| Question | Answer |
|---|---|
| Form Name | Form Dph 4192 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Immunization Form form dph 4192 |
DEPARTMENT OF HEALTH & FAMILY SERVICES |
|
STATE OF WISCONSIN |
Division of Public Health |
DAY CARE IMMUNIZATION RECORD |
ss. 252.04,Wis. Stats. |
DPH 4192 (Rev. 02/08) |
|
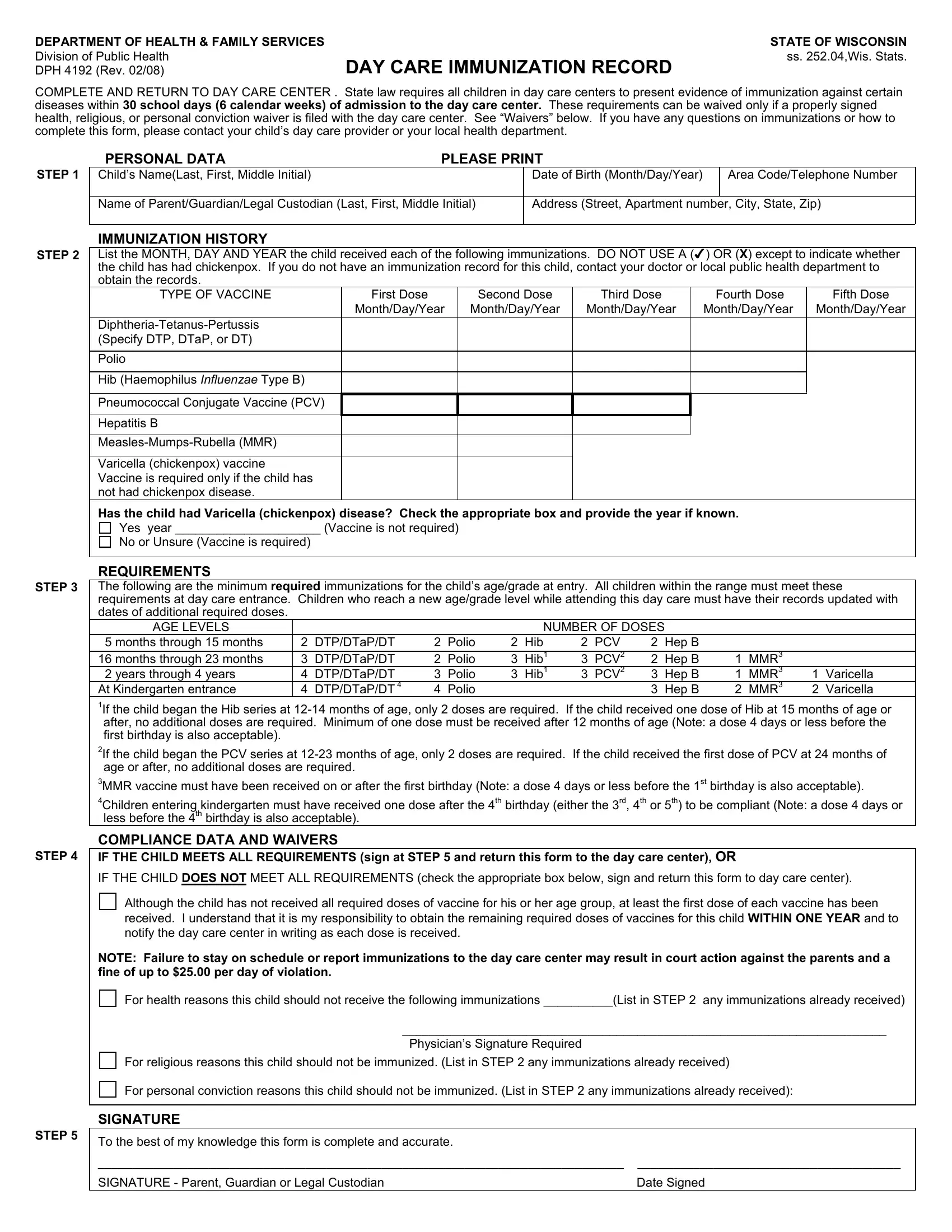
COMPLETE AND RETURN TO DAY CARE CENTER . State law requires all children in day care centers to present evidence of immunization against certain diseases within 30 school days (6 calendar weeks) of admission to the day care center. These requirements can be waived only if a properly signed health, religious, or personal conviction waiver is filed with the day care center. See “Waivers” below. If you have any questions on immunizations or how to complete this form, please contact your child’s day care provider or your local health department.
STEP 1
PERSONAL DATA |
PLEASE PRINT |
|
Child’s Name(Last, First, Middle Initial) |
Date of Birth (Month/Day/Year) |
Area Code/Telephone Number |
|
|
|
Name of Parent/Guardian/Legal Custodian (Last, First, Middle Initial)
Address (Street, Apartment number, City, State, Zip)
STEP 2
STEP 3
STEP 4
STEP 5
IMMUNIZATION HISTORY
List the MONTH, DAY AND YEAR the child received each of the following immunizations. DO NOT USE A ( ) OR (X) except to indicate whether the child has had chickenpox. If you do not have an immunization record for this child, contact your doctor or local public health department to obtain the records.
TYPE OF VACCINE |
First Dose |
Second Dose |
Third Dose |
Fourth Dose |
Fifth Dose |
|
Month/Day/Year |
Month/Day/Year |
Month/Day/Year |
Month/Day/Year |
Month/Day/Year |
|
|
|
|
|
|
(Specify DTP, DTaP, or DT) |
|
|
|
|
|
|
|
|
|
|
|
Polio |
|
|
|
|
|
|
|
|
|
|
|
Hib (Haemophilus INFLUENZAE Type B) |
|
|
|
|
|
|
|
|
|
|
|
Pneumococcal Conjugate Vaccine (PCV) |
|
|
|
|
|
|
|
|
|
|
|
Hepatitis B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Varicella (chickenpox) vaccine |
|
|
|
|
|
Vaccine is required only if the child has |
|
|
|
|
|
not had chickenpox disease. |
|
|
|
|
|
Has the child had Varicella (chickenpox) disease? Check the appropriate box and provide the year if known.
Yes year _____________________ (Vaccine is not required)
No or Unsure (Vaccine is required)
REQUIREMENTS
The following are the minimum required immunizations for the child’s age/grade at entry. All children within the range must meet these requirements at day care entrance. Children who reach a new age/grade level while attending this day care must have their records updated with dates of additional required doses.
AGE LEVELS |
|
|
|
|
|
NUMBER OF DOSES |
|
|
|
|
|||||
5 months through |
15 months |
2 |
DTP/DTaP/DT |
2 |
Polio |
2 |
Hib |
2 |
PCV |
2 |
Hep B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16 months through |
23 months |
3 |
DTP/DTaP/DT |
2 |
Polio |
3 |
Hib1 |
3 |
PCV2 |
2 |
Hep B |
1 |
MMR3 |
|
|
2 years through 4 years |
4 |
DTP/DTaP/DT |
3 |
Polio |
3 |
Hib1 |
3 |
PCV2 |
3 |
Hep B |
1 |
MMR3 |
1 |
Varicella |
|
At Kindergarten entrance |
4 |
DTP/DTaP/DT 4 |
4 |
Polio |
|
|
|
|
3 |
Hep B |
2 |
MMR3 |
2 |
Varicella |
|
1If the child began the Hib series at
2If the child began the PCV series at
3MMR vaccine must have been received on or after the first birthday (Note: a dose 4 days or less before the 1st birthday is also acceptable).
4Children entering kindergarten must have received one dose after the 4th birthday (either the 3rd, 4th or 5th) to be compliant (Note: a dose 4 days or less before the 4th birthday is also acceptable).
COMPLIANCE DATA AND WAIVERS
IF THE CHILD MEETS ALL REQUIREMENTS (sign at STEP 5 and return this form to the day care center), OR
IF THE CHILD DOES NOT MEET ALL REQUIREMENTS (check the appropriate box below, sign and return this form to day care center).
Although the child has not received all required doses of vaccine for his or her age group, at least the first dose of each vaccine has been received. I understand that it is my responsibility to obtain the remaining required doses of vaccines for this child WITHIN ONE YEAR and to notify the day care center in writing as each dose is received.
NOTE: Failure to stay on schedule or report immunizations to the day care center may result in court action against the parents and a fine of up to $25.00 per day of violation.
For health reasons this child should not receive the following immunizations __________(List in STEP 2 any immunizations already received)
______________________________________________________________________
Physician’s Signature Required
For religious reasons this child should not be immunized. (List in STEP 2 any immunizations already received)
For personal conviction reasons this child should not be immunized. (List in STEP 2 any immunizations already received):
SIGNATURE
To the best of my knowledge this form is complete and accurate. |
|
____________________________________________________________________________ |
______________________________________ |
SIGNATURE - Parent, Guardian or Legal Custodian |
Date Signed |