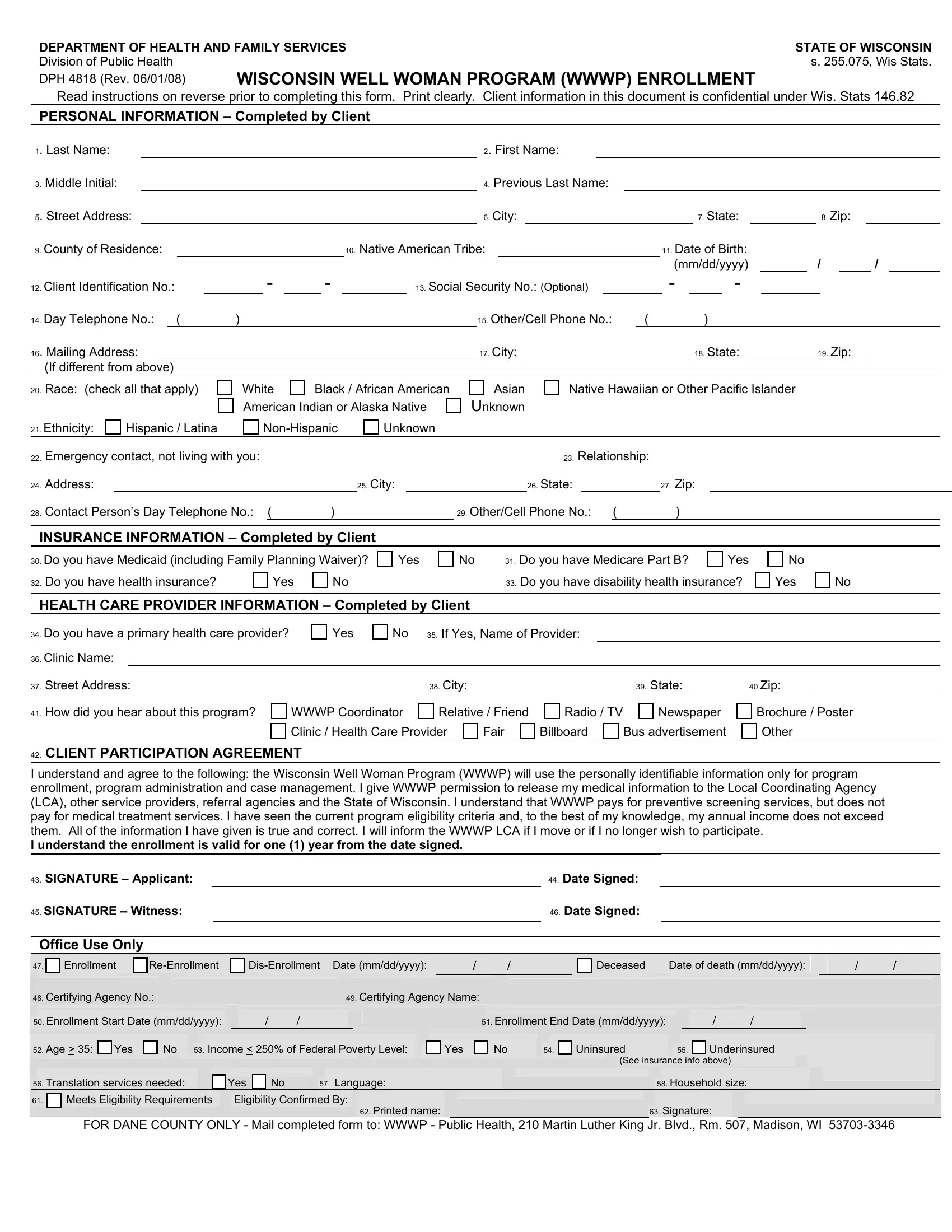
The DPH 4818 form serves as an essential document for the Wisconsin Well Woman Program (WWWP), an initiative by the Department of Health and Family Services within the State of Wisconsin. Directed towards the Division of Public Health under s. 255.075, Wis Stats, and updated last in June 2008, this form is pivotal for enrolling participants seeking preventive health screening services. It meticulously collects personal information, acknowledging the confidentiality protected under Wis. Stats 146.82, and covers a broad spectrum, from demographic details to insurance information, thus ensuring a comprehensive understanding of the applicant's eligibility and needs. Additionally, it includes a client participation agreement, emphasizing informed consent and the conditions of the program, like the coverage of preventive services but not medical treatment services, and stipulates the need for accurate and up-to-date information. The form becomes a crucial step for applicants to access the program's benefits, requiring thorough completion and an understanding of the WWWP's scope, enrollment process, and participant responsibilities. Through sections requesting details on healthcare providers and means of learning about the program, it also offers insights into the participant's healthcare journey and information dissemination effectiveness of the WWWP.
| Question | Answer |
|---|---|
| Form Name | Form Dph 4818 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Wis, Underinsured, Rm, LCA |
