
You are able to fill out SUBMITTING effectively in our PDFinity® editor. The tool is constantly updated by our staff, getting new awesome functions and growing to be even more versatile. Here's what you would have to do to get going:
Step 1: Click the "Get Form" button in the top area of this page to access our editor.
Step 2: After you access the PDF editor, you'll notice the document ready to be filled out. Besides filling out various blanks, you may also perform other things with the PDF, particularly writing custom words, changing the initial textual content, inserting illustrations or photos, placing your signature to the PDF, and a lot more.
If you want to fill out this PDF form, make sure that you enter the right details in every blank:
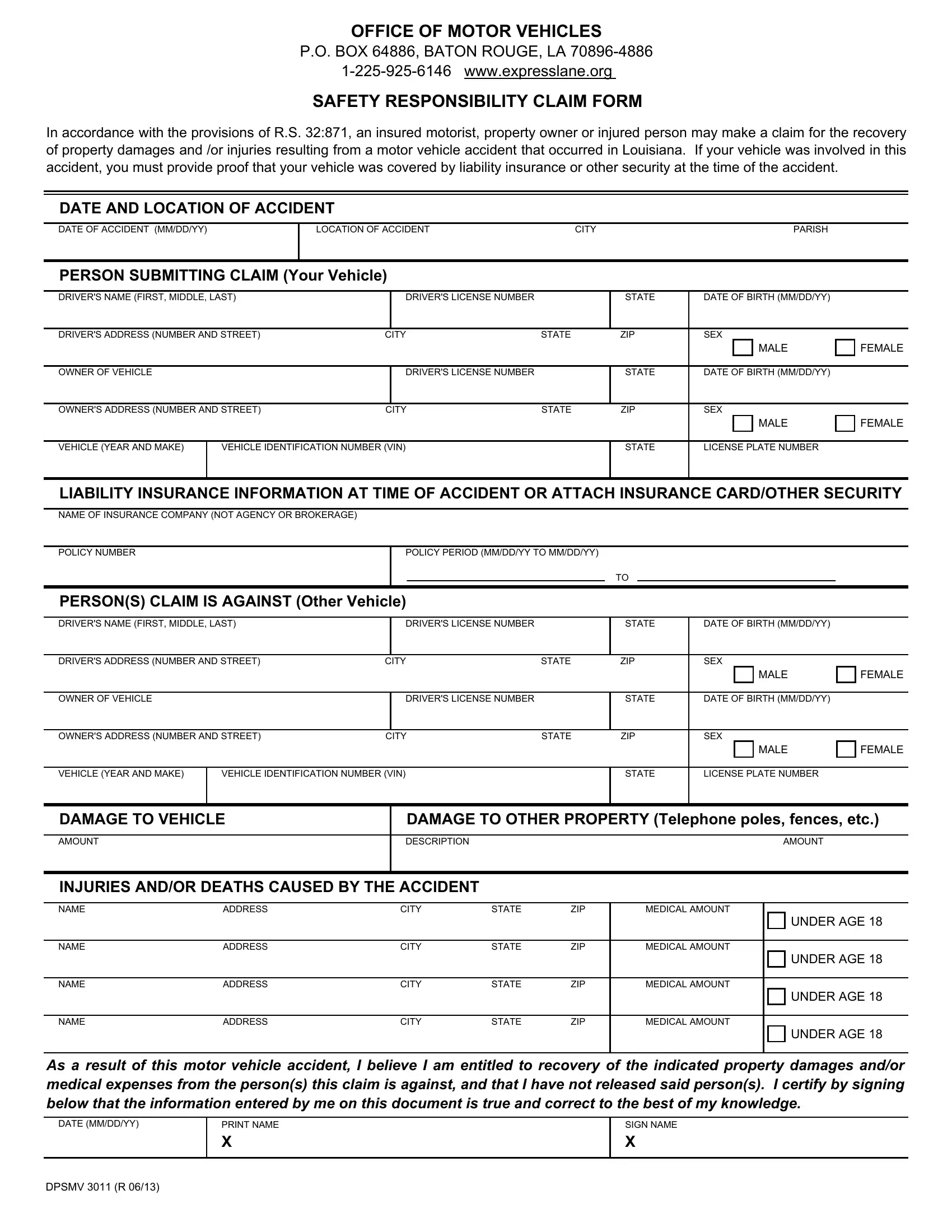
1. Fill out the SUBMITTING with a number of necessary fields. Consider all of the information you need and make sure nothing is omitted!
2. Your next step is usually to complete these blank fields: OWNER OF VEHICLE, DRIVERS LICENSE NUMBER, STATE, DATE OF BIRTH MMDDYY, OWNERS ADDRESS NUMBER AND STREET, SEX MALE FEMALE, VEHICLE YEAR AND MAKE, VEHICLE IDENTIFICATION NUMBER VIN, STATE, LICENSE PLATE NUMBER, DAMAGE TO VEHICLE, DAMAGE TO OTHER PROPERTY Telephone, AMOUNT, DESCRIPTION AMOUNT, and INJURIES ANDOR DEATHS CAUSED BY.
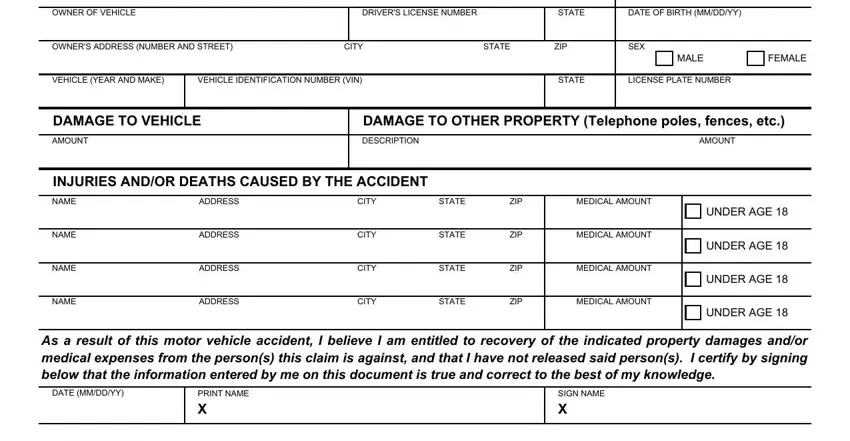
It is easy to get it wrong when filling in the DAMAGE TO VEHICLE, and so be sure you reread it before you'll submit it.
Step 3: When you've looked once again at the information entered, press "Done" to finalize your document generation. Try a 7-day free trial account at FormsPal and acquire direct access to SUBMITTING - which you can then work with as you wish in your FormsPal account. At FormsPal, we endeavor to make sure that all of your details are maintained secure.