
 Yes
Yes  No
No

 Yes
Yes  No
No
 Uncertain
Uncertain

 Yes
Yes  No
No
 Yes
Yes  No
No

 Yes
Yes  No
NoThe procedure of completing the form ds 326 is rather uncomplicated. Our team ensured our PDF editor is not difficult to utilize and helps prepare just about any PDF in a short time. Below are several steps you need to follow:
Step 1: Choose the button "Get form here" to get into it.
Step 2: Right now, you can begin editing the form ds 326. Our multifunctional toolbar is available to you - add, remove, adjust, highlight, and conduct several other commands with the words and phrases in the form.
Prepare the following parts to complete the file:
Remember to fill up the I certify or declare under penalty, DRIVERS SIGNATURE X, SECTION DRIVERS ADVISORY, All records of the DMV relating to, The department has sole, SECTION MEDICAL INFORMATION, DATE, MEDICAL RECORDPATIENT FILE NO, I hereby authorize my medical, I hereby authorize the DMV to, NOTE You may wish to make a copy, DATE, DS REV WWW, and Page of box with the expected details.
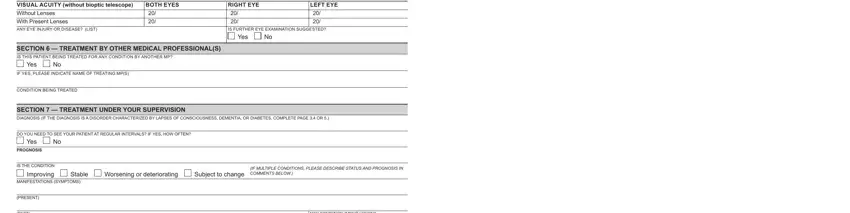
The application will require data to automatically fill up the field SECTION VISION VISUAL ACUITY, With Present Lenses ANY EYE INJURY, BOTH EYES, SECTION TREATMENT BY OTHER, Yes, IF YES PLEASE INDICATE NAME OF, CONDITION BEING TREATED, RIGHT EYE, LEFT EYE, IS FURTHER EYE EXAMINATION, Yes, SECTION TREATMENT UNDER YOUR, DO YOU NEED TO SEE YOUR PATIENT AT, Yes PROGNOSIS, and IS THE CONDITION.
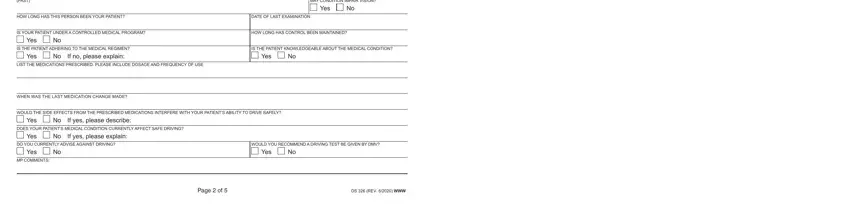
The PAST, MAY CONDITION IMPAIR VISION, Yes, HOW LONG HAS THIS PERSON BEEN YOUR, DATE OF LAST EXAMINATION, IS YOUR PATIENT UNDER A CONTROLLED, HOW LONG HAS CONTROL BEEN, Yes, IS THE PATIENT ADHERING TO THE, Yes, If no please explain, LIST THE MEDICATIONS PRESCRIBED, IS THE PATIENT KNOWLEDGEABLE ABOUT, Yes, and WHEN WAS THE LAST MEDICATION segment can be used to indicate the rights and responsibilities of either side.
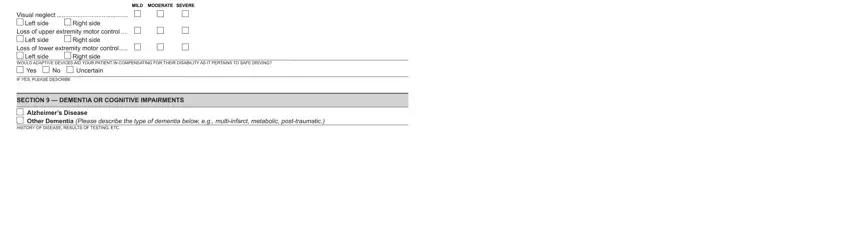
Finish by reading these sections and filling out the proper information: Functional impairments that may, MILD MODERATE SEVERE, Visual neglect, Left side, Right side, Loss of upper extremity motor, Left side, Right side, Loss of lower extremity motor, Left side, Right side, WOULD ADAPTIVE DEVICES AID YOUR, Yes, Uncertain, and IF YES PLEASE DESCRIBE.
Step 3: Click "Done". It's now possible to upload your PDF form.
Step 4: Come up with a duplicate of every form. It may save you time and permit you to stay clear of worries later on. Keep in mind, your data isn't going to be shared or analyzed by us.
