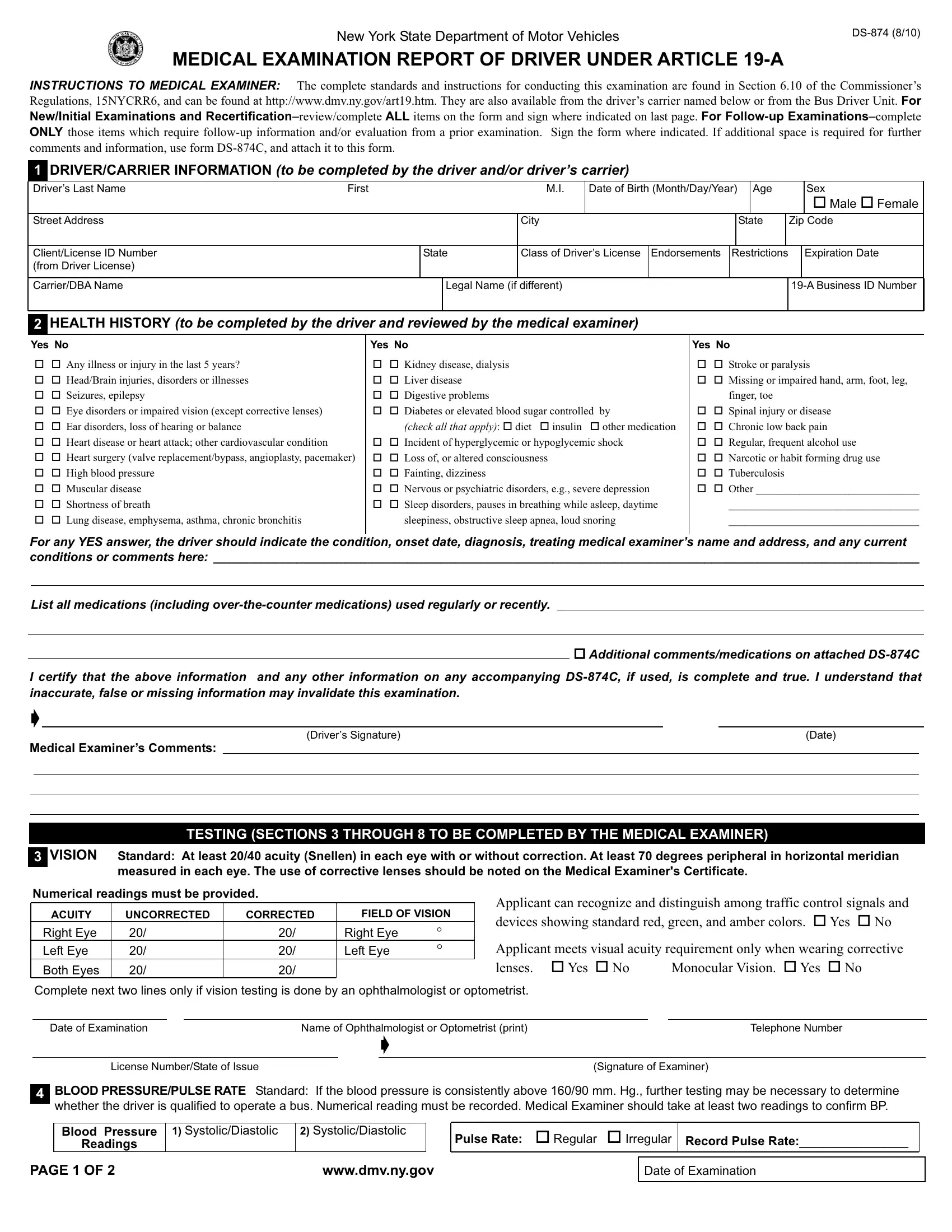
Ensuring the safety of both passengers and drivers on the road is paramount, and the New York State Department of Motor Vehicles takes this responsibility seriously through the implementation of the Medical Examination Report for Driver Under Article 19-A, known as the DS-874 form. This comprehensive form is a vital tool designed to assess the physical and medical fitness of commercial bus drivers, aiming to prevent health-related incidents that could compromise public safety. It encompasses a thorough examination and health history review, ranging from vision and hearing tests to cardiovascular health, diabetes management, and neurologic conditions. Medical examiners are tasked with completing this form with considerable care, adhering to the specific standards and instructions outlined in Section 6.10 of the Commissioner’s Regulations, 15NYCRR6. Whether it's a new applicant seeking certification or a seasoned driver undergoing recertification or follow-up, this form serves as a crucial checkpoint in ensuring that drivers possess the necessary physical and mental health standards to safely operate a commercial vehicle. Additionally, modifications or restrictions, such as the requirement for corrective lenses or hearing aids, are clearly identified to tailor the certification to the driver’s specific needs, ensuring that all those behind the wheel are not only legally compliant but also medically equipped to handle the demands of their role.
| Question | Answer |
|---|---|
| Form Name | Form Ds 874 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | bruits, 500Hz, 19-A, genetic medical examination form |
