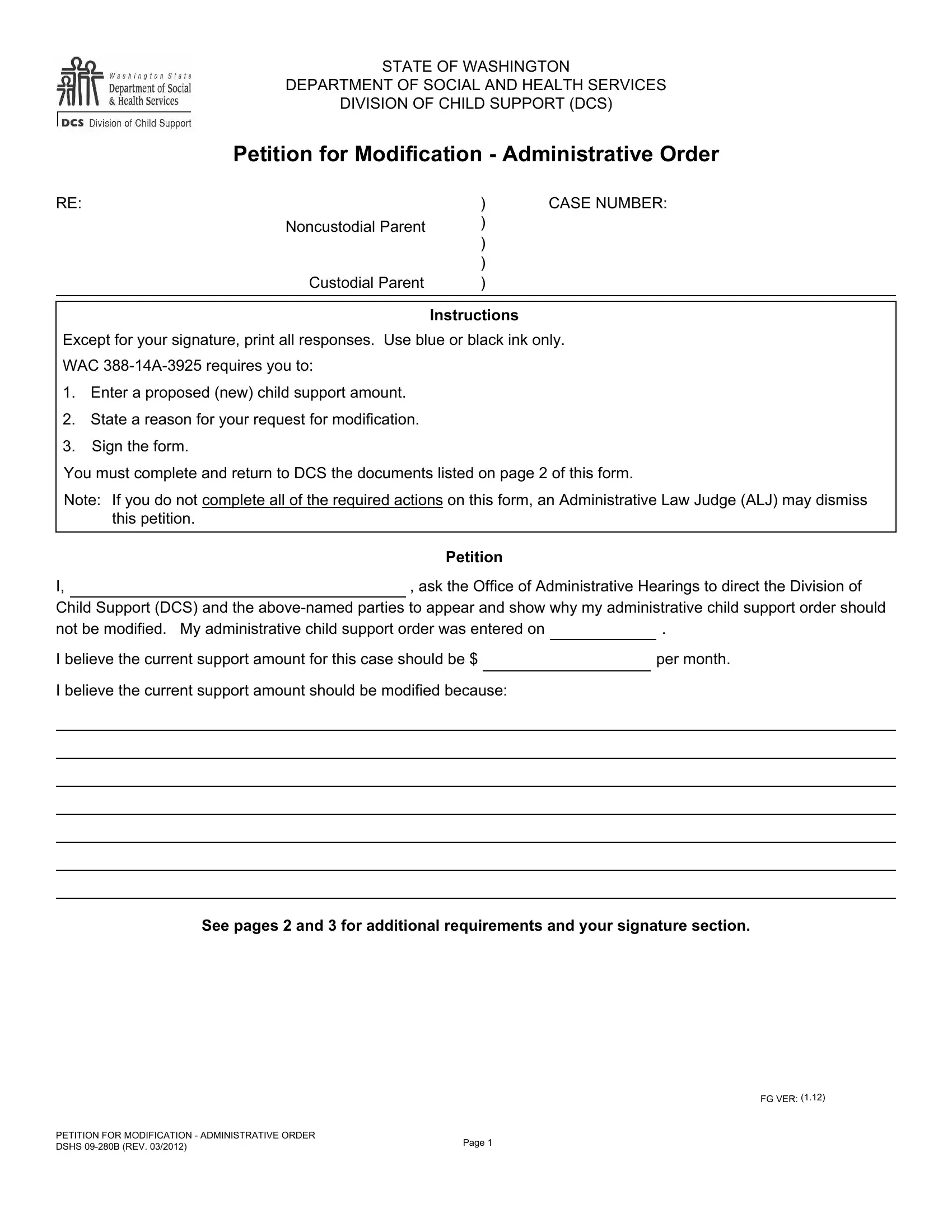
Navigating the complexities of child support modification in the state of Washington is facilitated through the use of the DSHS 09 280B form, a key document provided by the Department of Social and Health Services, Division of Child Support (DCS). This form serves as a petition for individuals seeking to modify an existing administrative child support order. It outlines a clearly structured process requiring petitioners to propose a new child support amount, state the reasons for the modification request, and obligates them to adhere to specific documentation and procedural requirements. The form emphasizes the importance of providing a detailed rationale for the modification, backed by a signature that attests to the truthfulness of the provided information. Additionally, it highlights the critical role of the Administrative Law Judge (ALJ) who may dismiss the petition if all required actions, as stipulated on the form, are not completed. Furthermore, it addresses circumstances under which the DCS might oppose the petition, outlines obligations related to health insurance provision for the child or children involved, and sets forth the expectations from both custodial and noncustodial parents in terms of documentation and communication with the DCS. This petition form embodies a crucial step for parents in the modification of a child support order, necessitating a clear understanding and precise compliance with its outlined requirements.
| Question | Answer |
|---|---|
| Form Name | Form Dshs 09 280B |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | 09 280b child support forms wa 09 280b |
STATE OF WASHINGTON
DEPARTMENT OF SOCIAL AND HEALTH SERVICES
DIVISION OF CHILD SUPPORT (DCS)
Petition for Modification - Administrative Order
RE: |
) |
CASE NUMBER: |
Noncustodial Parent |
) |
|
|
|
|
|
) |
|
|
) |
|
Custodial Parent |
) |
|
|
|
|
Instructions
Except for your signature, print all responses. Use blue or black ink only.
WAC
1.Enter a proposed (new) child support amount.
2.State a reason for your request for modification.
3.Sign the form.
You must complete and return to DCS the documents listed on page 2 of this form.
Note: If you do not complete all of the required actions on this form, an Administrative Law Judge (ALJ) may dismiss this petition.
|
Petition |
I, |
, ask the Office of Administrative Hearings to direct the Division of |
Child Support (DCS) and the
not be modified. My administrative child support order was entered on |
. |
|||
I believe the current support amount for this case should be $ |
|
|
per month. |
|
|
|
|
|
|
I believe the current support amount should be modified because: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
See pages 2 and 3 for additional requirements and your signature section.
FG VER: (1.12)
PETITION FOR MODIFICATION - ADMINISTRATIVE ORDER |
Page 1 |
|
DSHS |
||
|
Acknowledgements
I understand that:
1.DCS will oppose this petition if it does not meet the criteria for modifying an order contained in RCW 74.20A.059.
2.If my order does not now contain these provisions, DCS will ask the ALJ to include provisions in my order requiring each parent to provide health insurance coverage for the child(ren) if coverage is now or becomes available through employment or a union and the health insurance premium does not exceed 25 percent of the parent's basic support obligation. DCS considers this requirement satisfied if the child(ren) is / are eligible for Indian Health Services. DCS may enforce this obligation under certain circumstances. The obligated parent must provide proof of accessible coverage for the child(ren) to DCS and the other parent within 20 days of the date a final child support order is entered. If the obligated parent does not provide proof of coverage, the obligated parent may be required to satisfy the obligation to provide health insurance by doing one of the following, in order of priority:
a.Providing or maintaining health insurance coverage through the obligated parent's employment or union at a cost not to exceed 25 percent of the obligated parent's basic child support obligation.
b.Contributing the obligated parent's proportionate share of a monthly premium being paid by the other parent for health insurance coverage for the child(ren) named in the support order, not to exceed 25 percent of the obligated parent's basic child support obligation.
c.The noncustodial parent may be required to contribute a proportionate share of a monthly premium being paid by the state, not to exceed 25 percent of the noncustodial parent's basic child support obligation, if the child(ren) receive(s)
3.I must ask for a specific amount of child support, provide a reason for requesting the modification, and sign this form. If I do not, DCS cannot process my petition.
4.I must file the following documents with DCS:
a.This completed petition.
b.Completed Washington State Child Support Schedule worksheets.
c.If I am a parent of the child(ren), proof of income (pay stubs, tax returns, etc.).
5.I must mail the above documents to the following address or personally deliver them to the DCS office that handles my case. DIVISION OF CHILD SUPPORT
PO BOX 11520 TACOMA WA
6.If I do not provide the above documents to DCS, an ALJ may dismiss my petition.
7.I must tell DCS if I change my address.
8.I must tell DCS of any changes in health insurance coverage for my child(ren).
9.DCS does not represent me or the other party to my child support order in this action.
10.If I do not attend and participate in a scheduled hearing, an ALJ may dismiss my petition.
11.If the other party to my order does not attend and participate in a scheduled hearing, an ALJ may:
a.Grant any requests made by DCS or the appearing party to the case without further notice.
b.Order a support amount that is higher or lower than the amount proposed in this petition.
FG VER: (1.12)
PETITION FOR MODIFICATION - ADMINISTRATIVE ORDER |
Page 2 |
|
DSHS |
||
|
Notice to Both Parents
An ALJ may:
1.Order both parents to provide health insurance for the child(ren) if coverage is now or becomes available through employment or a union and the health insurance premium does not exceed 25 percent of the parents' basic child support obligations.
2.Order both parents to pay a proportionate share of uninsured medical expenses, including copayments, deductibles, and any part of the proportionate share of a medical insurance premium not enforced through service of a Notice of Support Owed.
3.Order that if a parent who is ordered to provide health insurance coverage for the child(ren) does not provide proof of accessible coverage, DCS may do one of the following, listed in order of priority:
a.Send a notice to the employer or union requiring the employer or union to enroll the child(ren) in a health insurance plan as described in RCW 28.18.170.
b.Serve a notice on the obligated parent requiring the parent to pay his / her proportionate share of a monthly premium being paid by the other parent for the child(ren), not to exceed 25 percent of the obligated parent's basic child support obligation; or
c.Serve a notice on the obligated parent requiring the parent to contribute to his / her proportionate share of a monthly premium paid by the state, not to exceed 25 percent of the obligated parent's basic child support obligation, if the child(ren) receive(s)
4.Order that if an obligated parent fails to enroll the child(ren) in accessible health insurance coverage, or coverage available through the parent's employer or union, DCS may enforce the obligated parent's medical support obligation as provided in RCW 26.18.170.
Declaration
I declare, under penalty of perjury under the laws of the state of Washington, that the foregoing is true and correct.
You must sign this form
DATE
P.O. BOX OR STREET ADDRESS
CITYSTATEZIP CODE
( |
) |
|
( |
) |
|
HOME TELEPHONE NUMBER |
|
CELL TELEPHONE NUMBER |
|||
( |
) |
|
( |
) |
|
|
|
||||
|
|
|
|
||
WORK TELEPHONE NUMBER |
|
MESSAGE TELEPHONE NUMBER |
|||
( |
) |
|
|
|
|
FAX NUMBER
BEST HOURS TO CALL ME
NUMBER I PREFER TO USE FOR THE HEARING
MY SIGNATURE
MY ATTORNEY'S OR REPRESENTATIVE'S NAME
MY ATTORNEY'S OR REPRESENTATIVE'S ADDRESS
MY ATTORNEY'S OR REPRESENTATIVE'S CITY, STATE, ZIP CODE
()
MY ATTORNEY'S OR REPRESENTATIVE'S TELEPHONE NUMBER
No person, because of race, color, national origin, creed, religion, sex, age, or disability, shall be discriminated against in employment, services, or any aspect of the program's activities. This form is available in alternative formats upon request.
FG VER: (1.12)
PETITION FOR MODIFICATION - ADMINISTRATIVE ORDER |
Page 3 |
|
DSHS |
||
|