
 PER FAMILY
PER FAMILY

 Yes
Yes 
 No If yes to #2, please check the box below that applies to you.
No If yes to #2, please check the box below that applies to you.
 Yes
Yes 
 No
NoThe procedure of filling out the BIRTHDATE is quite easy. Our experts made sure our tool is not hard to work with and can help fill out almost any document in no time. The following are a few steps you will need to follow:
Step 1: Choose the orange "Get Form Now" button on this website page.
Step 2: So you're on the file editing page. You can modify and add content to the file, highlight specified content, cross or check certain words, add images, insert a signature on it, get rid of needless fields, or eliminate them altogether.
These areas are within the PDF form you will be filling out.
Put the asked particulars in the Please call the number below if, Call Center Telephone Number, Fax Number, and CCSP APPLICATION DSHS REV part.
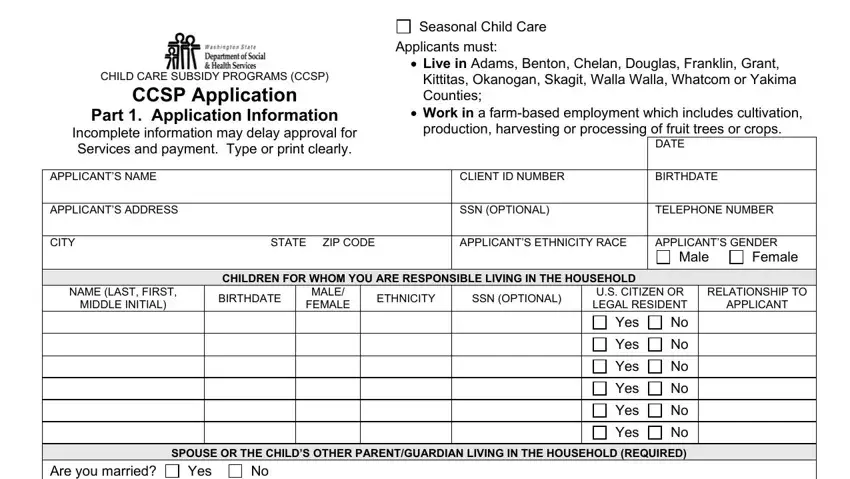
You should be demanded specific relevant details if you want to prepare the Seasonal Child Care, Applicants must, CHILD CARE SUBSIDY PROGRAMS CCSP, Live in Adams Benton Chelan, Kittitas Okanogan Skagit Walla, Work in a farmbased employment, DATE, APPLICANTS NAME, CLIENT ID NUMBER, BIRTHDATE, APPLICANTS ADDRESS, SSN OPTIONAL, TELEPHONE NUMBER, CITY, and STATE ZIP CODE box.
The NAME, BIRTHDATE, SSN OPTIONAL, RELATIONSHIP TO APPLICANT, RELATIONSHIP TO ABOVE CHILDREN, NAME OF EMPLOYER WORKFIRST, NAME OF EMPLOYER WORKFIRST, APPLICANT, SPOUSE OR SECOND PARENTGUARDIAN, ADDRESS EMPLOYMENT WORKFIRST, ADDRESS EMPLOYMENT WORKFIRST, TELEPHONE NUMBER, DATE STARTED, TELEPHONE NUMBER, and DATE STARTED field will be your place to indicate the rights and responsibilities of both sides.
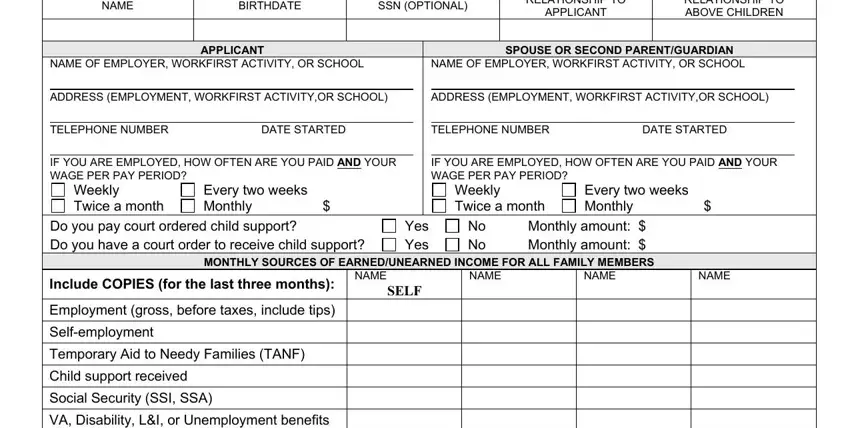
Check the fields VA Disability LI or Unemployment and then fill them out.

Step 3: Click the Done button to assure that your finalized form is available to be exported to every gadget you select or mailed to an email you indicate.
Step 4: Make sure you avoid future troubles by producing no less than a pair of copies of your file.
