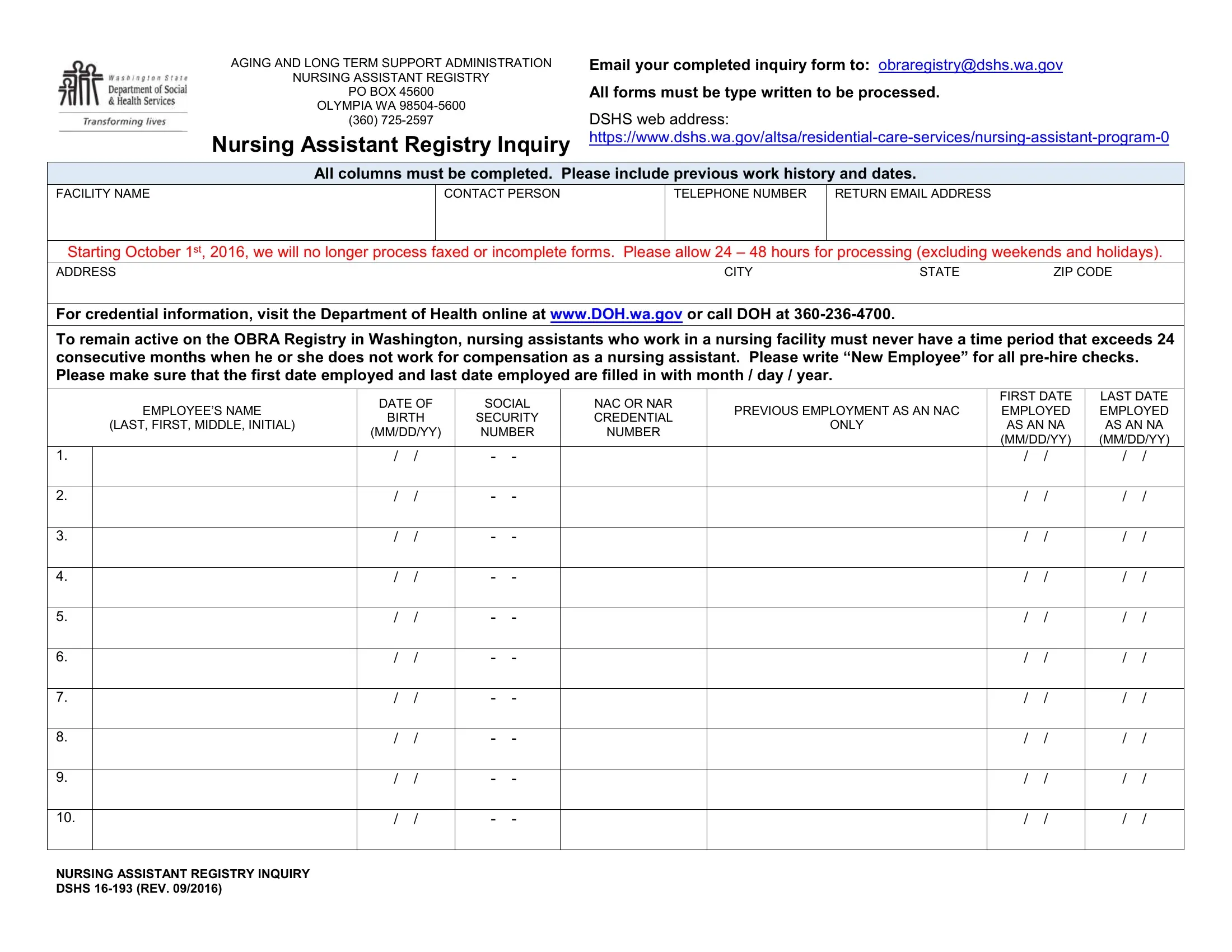
Navigating through the intricacies of healthcare administration and compliance can often feel like an overwhelming task, especially when it comes to maintaining the qualifications and credentials of healthcare personnel. Enter the DSHS 16-193 form, a critical piece of documentation utilized by the Aging and Long Term Support Administration that serves a pivotal role in this complex landscape. This form is expressly designed for the Nursing Assistant Registry in Washington State, required to be filled out and submitted by facilities wishing to inquire about the credentials of current or prospective nursing assistants. With a mandate that all entries be typewritten to facilitate processing, the form underscores the importance of accuracy and attention to detail in administrative healthcare tasks. It encompasses fields for detailed employment history, including specific dates of employment, which are crucial for ensuring that nursing assistants remain active on the OBRA Registry by meeting the requirement of not having a break in service exceeding 24 consecutive months. Furthermore, starting from October 1st, 2016, the administration has taken a firm stance against processing incomplete or faxed forms, thereby emphasizing the shift towards more secure and reliable electronic communication channels for such critical exchanges of information. This form not only acts as a gateway for verifying the credentials of nursing assistants via the Department of Health but also streamlines the hiring process by distinguishing between new and returning employees, thereby aiding in the efficient administration of long-term care facilities.
| Question | Answer |
|---|---|
| Form Name | Form Dshs 16 193 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | wa dshs aide, request identicard form online, dshs 16 234 wa, how to dshs inquiry |
AGING AND LONG TERM SUPPORT ADMINISTRATION |
Email your completed inquiry form to: obraregistry@dshs.wa.gov |
NURSING ASSISTANT REGISTRY |
|
PO BOX 45600 |
All forms must be type written to be processed. |
OLYMPIA WA |
|
(360) |
DSHS web address: |
Nursing Assistant Registry Inquiry |
All columns must be completed. Please include previous work history and dates.
FACILITY NAME
CONTACT PERSON
TELEPHONE NUMBER |
RETURN EMAIL ADDRESS |
|
|
Starting October 1st, 2016, we will no longer process faxed or incomplete forms. Please allow 24 – 48 hours for processing (excluding weekends and holidays).
ADDRESS |
CITY |
STATE |
ZIP CODE |
For credential information, visit the Department of Health online at www.DOH.wa.gov or call DOH at
To remain active on the OBRA Registry in Washington, nursing assistants who work in a nursing facility must never have a time period that exceeds 24 consecutive months when he or she does not work for compensation as a nursing assistant. Please write “New Employee” for all
|
|
DATE OF |
SOCIAL |
NAC OR NAR |
|
FIRST DATE |
LAST DATE |
||||
|
EMPLOYEE’S NAME |
PREVIOUS EMPLOYMENT AS AN NAC |
EMPLOYED |
EMPLOYED |
|||||||
|
BIRTH |
SECURITY |
CREDENTIAL |
||||||||
|
(LAST, FIRST, MIDDLE, INITIAL) |
ONLY |
AS AN NA |
AS AN NA |
|||||||
|
(MM/DD/YY) |
NUMBER |
NUMBER |
||||||||
|
|
|
(MM/DD/YY) |
(MM/DD/YY) |
|||||||
|
|
|
|
|
|
|
|
||||
1. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
6. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
7. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
8. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
9. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
10. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
NURSING ASSISTANT REGISTRY INQUIRY DSHS