Since the early 1900s, the Texas Department of State Health Services (Dshs) has been working to improve the health and well-being of all Texans. Form Dshs 16 193 is one of the many ways that this agency fulfills its mission. This form is used by medical professionals to report cases of suspected tuberculosis (TB) in Texas. Reporting potential cases of TB helps Dshs officials track and respond to outbreaks, as well as provide treatment for those who have the disease. Anyone who suspects they may have TB should consult a healthcare professional and complete Form Dshs 16 193. Knowing about this form and what it entails can help ensure that potential cases of TB are promptly reported and treated.
| Question | Answer |
|---|---|
| Form Name | Form Dshs 16 193 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | wa dshs aide, request identicard form online, dshs 16 234 wa, how to dshs inquiry |
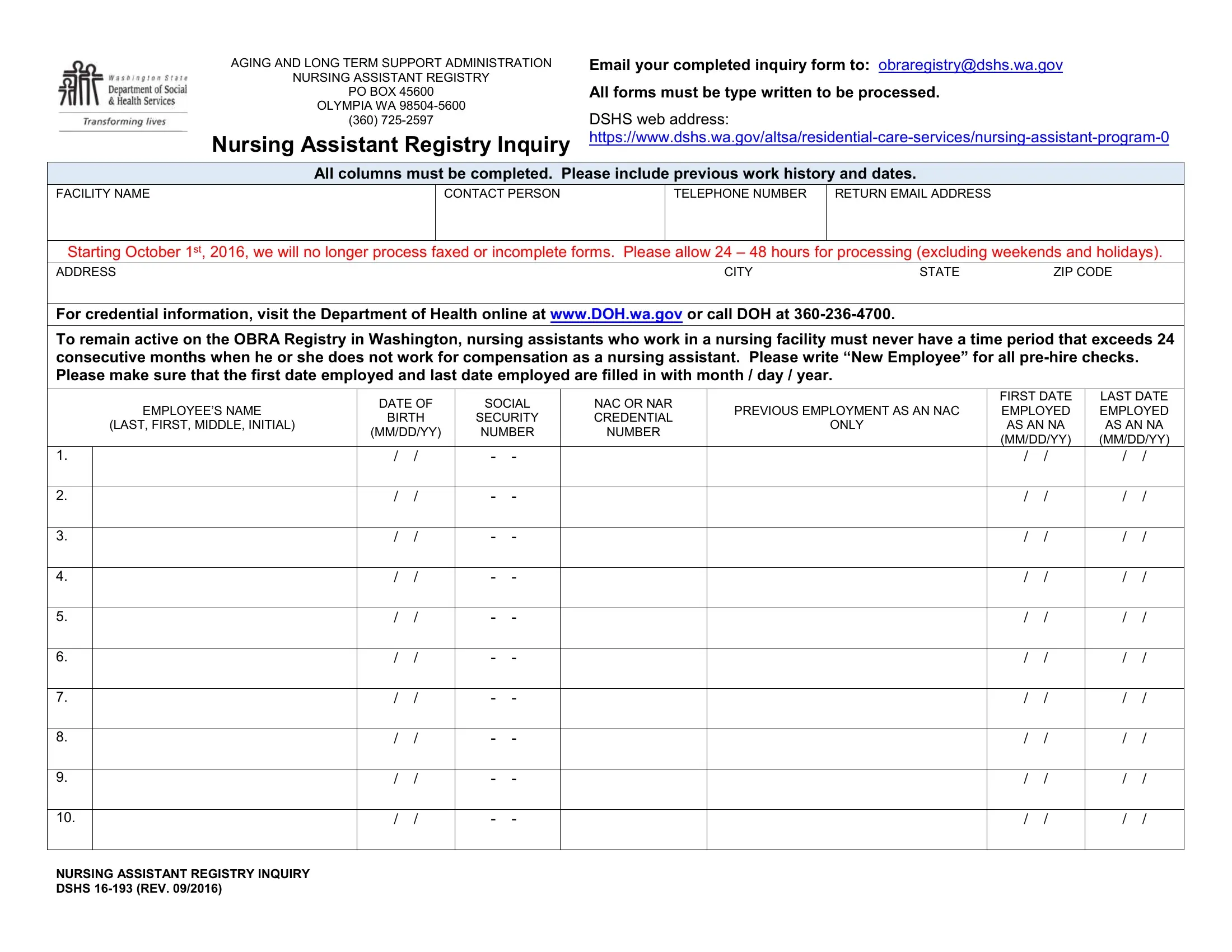
AGING AND LONG TERM SUPPORT ADMINISTRATION |
Email your completed inquiry form to: obraregistry@dshs.wa.gov |
NURSING ASSISTANT REGISTRY |
|
PO BOX 45600 |
All forms must be type written to be processed. |
OLYMPIA WA |
|
(360) |
DSHS web address: |
Nursing Assistant Registry Inquiry |
All columns must be completed. Please include previous work history and dates.
FACILITY NAME
CONTACT PERSON
TELEPHONE NUMBER |
RETURN EMAIL ADDRESS |
|
|
Starting October 1st, 2016, we will no longer process faxed or incomplete forms. Please allow 24 – 48 hours for processing (excluding weekends and holidays).
ADDRESS |
CITY |
STATE |
ZIP CODE |
For credential information, visit the Department of Health online at www.DOH.wa.gov or call DOH at
To remain active on the OBRA Registry in Washington, nursing assistants who work in a nursing facility must never have a time period that exceeds 24 consecutive months when he or she does not work for compensation as a nursing assistant. Please write “New Employee” for all
|
|
DATE OF |
SOCIAL |
NAC OR NAR |
|
FIRST DATE |
LAST DATE |
||||
|
EMPLOYEE’S NAME |
PREVIOUS EMPLOYMENT AS AN NAC |
EMPLOYED |
EMPLOYED |
|||||||
|
BIRTH |
SECURITY |
CREDENTIAL |
||||||||
|
(LAST, FIRST, MIDDLE, INITIAL) |
ONLY |
AS AN NA |
AS AN NA |
|||||||
|
(MM/DD/YY) |
NUMBER |
NUMBER |
||||||||
|
|
|
(MM/DD/YY) |
(MM/DD/YY) |
|||||||
|
|
|
|
|
|
|
|
||||
1. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
6. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
7. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
8. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
9. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
10. |
|
/ |
/ |
- |
- |
|
|
/ |
/ |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
NURSING ASSISTANT REGISTRY INQUIRY DSHS