
RI can be completed easily. Just open FormsPal PDF editor to accomplish the job right away. To have our tool on the forefront of practicality, we work to adopt user-driven features and improvements regularly. We are at all times looking for suggestions - play a vital part in reshaping the way you work with PDF documents. Starting is easy! All that you should do is follow these simple steps below:
Step 1: Click on the "Get Form" button at the top of this page to access our editor.
Step 2: The tool will let you change PDF files in various ways. Enhance it by including personalized text, correct what's already in the file, and place in a signature - all within a few mouse clicks!
It will be simple to complete the document using out detailed tutorial! This is what you have to do:
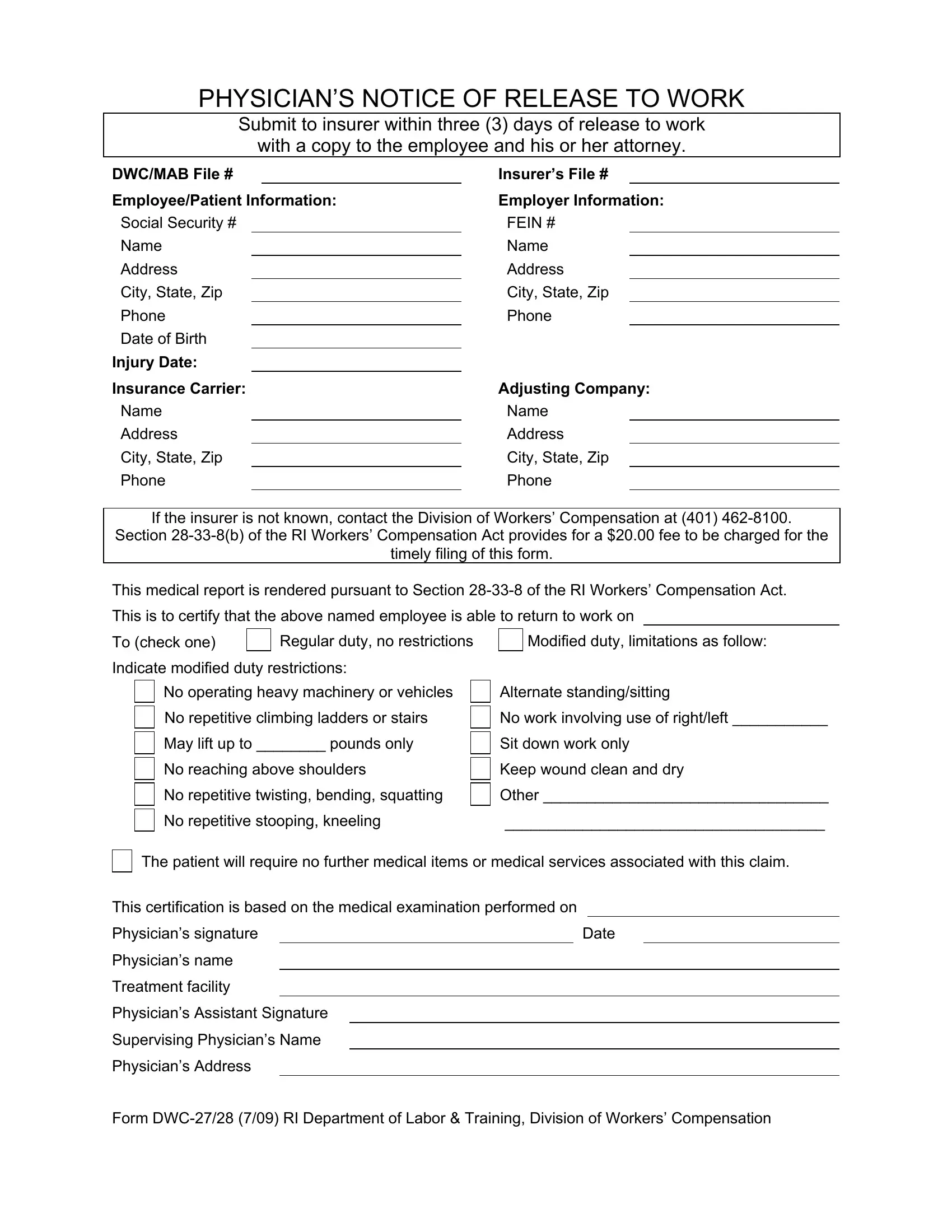
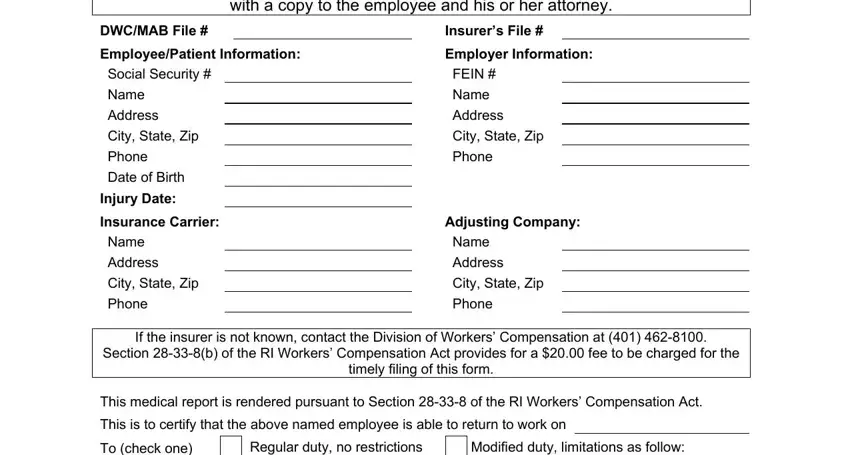
1. Firstly, once completing the RI, start out with the form section that features the next blanks:
2. The third stage would be to fill in the following fields: Indicate modified duty restrictions, No operating heavy machinery or, No work involving use of, May lift up to pounds only, Sit down work only, No reaching above shoulders, Keep wound clean and dry, No repetitive twisting bending, Other, No repetitive stooping kneeling, The patient will require no, This certification is based on the, Date, Physicians signature, and Physicians name.
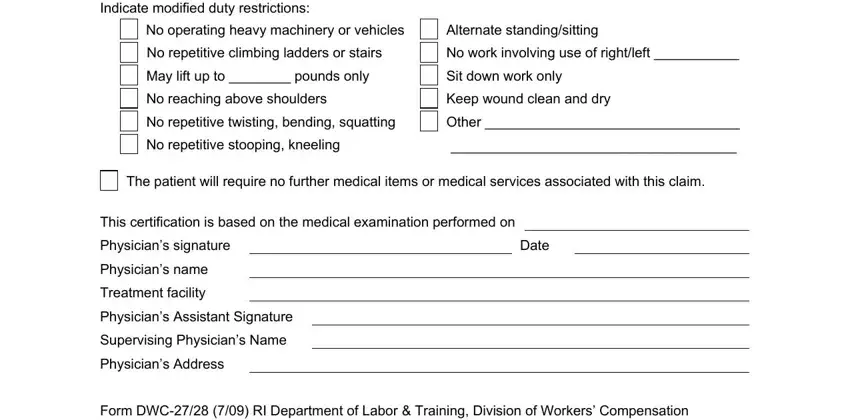
Be really mindful when completing This certification is based on the and No repetitive twisting bending, as this is the part in which most people make errors.
Step 3: After you've glanced through the information entered, simply click "Done" to conclude your form. Go for a free trial plan at FormsPal and obtain direct access to RI - with all transformations preserved and available from your personal cabinet. FormsPal is devoted to the personal privacy of all our users; we make sure all information coming through our system is confidential.