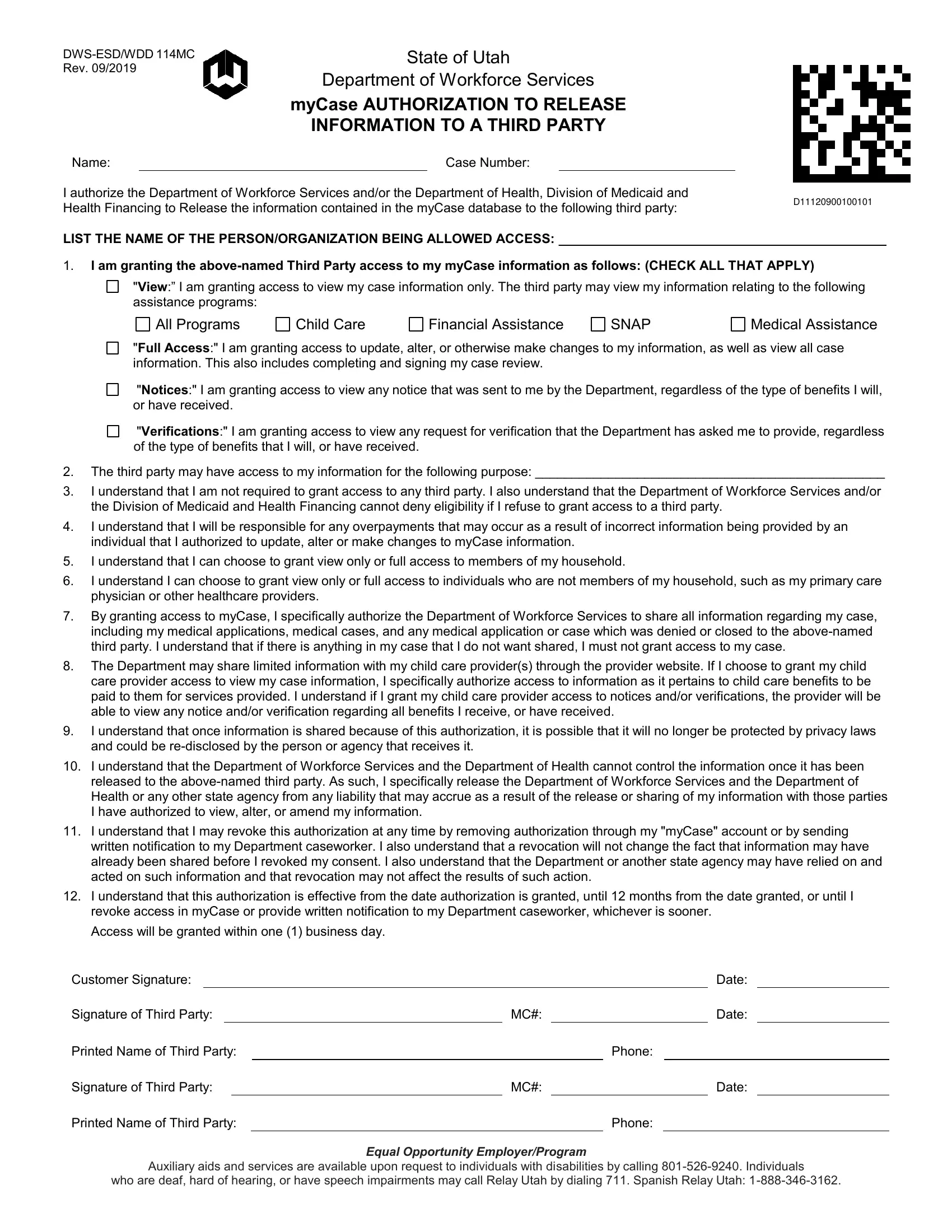
In an era where data privacy and security are paramount, the DWS-ESD/WDD 114MC form represents a crucial tool for individuals interacting with the State of Utah's Department of Workforce Services and the Department of Health, Division of Medicaid and Health Financing. This form serves as an authorization mechanism, allowing individuals to grant third parties access to their personal information within the myCase database, under specific conditions. The form outlines various access levels, ranging from viewing case information related to assistance programs like SNAP, Child Care Financial Assistance, and Medical Assistance to full access, which includes the ability to update or alter case information. It underscores the voluntary nature of this authorization, iterating that eligibility for services cannot be denied if one refuses to grant access. Moreover, the form highlights the responsibilities incumbent upon the individual, especially regarding potential overpayments due to inaccuracies submitted by the authorized third party. It contains explicit content on what granting access entails, including sharing sensitive medical information, conditions under which child care providers may access information, and the potential risks once information is shared. Importantly, it spells out the rights of individuals to revoke this authorization and specifies the protective measures that cease to apply once information is released, underlining the department's immunity from liability post-disclosure. Through this form, users navigate the complexities of information sharing, balancing the need for assistance with the imperative of maintaining control over their personal data.
| Question | Answer |
|---|---|
| Form Name | Form Dws Esd Wdd 114Mc |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Utah, revocation, dws mycase, eligibility |
State of Utah
Department of Workforce Services
myCase AUTHORIZATION TO RELEASE
INFORMATION TO A THIRD PARTY
Name:Case Number:
I authorize the Department of Workforce Services and/or the Department of Health, Division of Medicaid and
Health Financing to Release the information contained in the myCase database to the following third party: |
D11120900100101 |
|
|
LIST THE NAME OF THE PERSON/ORGANIZATION BEING ALLOWED ACCESS: _____________________________________________ |
|
1.I am granting the
"View:” I am granting access to view my case information only. The third party may view my information relating to the following assistance programs:
All Programs
Child Care
Financial Assistance
SNAP
Medical Assistance
"Full Access:" I am granting access to update, alter, or otherwise make changes to my information, as well as view all case information. This also includes completing and signing my case review.
"Notices:" I am granting access to view any notice that was sent to me by the Department, regardless of the type of benefits I will, or have received.
"Verifications:" I am granting access to view any request for verification that the Department has asked me to provide, regardless of the type of benefits that I will, or have received.
2.The third party may have access to my information for the following purpose: ________________________________________________
3.I understand that I am not required to grant access to any third party. I also understand that the Department of Workforce Services and/or the Division of Medicaid and Health Financing cannot deny eligibility if I refuse to grant access to a third party.
4.I understand that I will be responsible for any overpayments that may occur as a result of incorrect information being provided by an individual that I authorized to update, alter or make changes to myCase information.
5.I understand that I can choose to grant view only or full access to members of my household.
6.I understand I can choose to grant view only or full access to individuals who are not members of my household, such as my primary care physician or other healthcare providers.
7.By granting access to myCase, I specifically authorize the Department of Workforce Services to share all information regarding my case, including my medical applications, medical cases, and any medical application or case which was denied or closed to the
8.The Department may share limited information with my child care provider(s) through the provider website. If I choose to grant my child care provider access to view my case information, I specifically authorize access to information as it pertains to child care benefits to be paid to them for services provided. I understand if I grant my child care provider access to notices and/or verifications, the provider will be able to view any notice and/or verification regarding all benefits I receive, or have received.
9.I understand that once information is shared because of this authorization, it is possible that it will no longer be protected by privacy laws and could be
10.I understand that the Department of Workforce Services and the Department of Health cannot control the information once it has been released to the
11.I understand that I may revoke this authorization at any time by removing authorization through my "myCase" account or by sending written notification to my Department caseworker. I also understand that a revocation will not change the fact that information may have already been shared before I revoked my consent. I also understand that the Department or another state agency may have relied on and acted on such information and that revocation may not affect the results of such action.
12.I understand that this authorization is effective from the date authorization is granted, until 12 months from the date granted, or until I revoke access in myCase or provide written notification to my Department caseworker, whichever is sooner.
Access will be granted within one (1) business day.
Customer Signature: |
|
|
|
|
|
Date: |
|
|||
Signature of Third Party: |
|
MC#: |
|
|
|
Date: |
|
|||
Printed Name of Third Party: |
|
|
|
Phone: |
|
|||||
Signature of Third Party: |
|
MC#: |
|
|
|
Date: |
||||
Printed Name of Third Party: |
|
|
|
Phone: |
|
|||||
Equal Opportunity Employer/Program
Auxiliary aids and services are available upon request to individuals with disabilities by calling
who are deaf, hard of hearing, or have speech impairments may call Relay Utah by dialing 711. Spanish Relay Utah: