


Lic can be completed online very easily. Just use FormsPal PDF editor to do the job right away. To keep our tool on the forefront of efficiency, we aim to implement user-driven capabilities and enhancements regularly. We are at all times looking for feedback - play a vital part in revampimg PDF editing. With a few basic steps, you'll be able to begin your PDF journey:
Step 1: Press the "Get Form" button above. It is going to open up our pdf editor so that you can begin completing your form.
Step 2: The editor will let you work with the majority of PDF documents in a range of ways. Modify it by writing customized text, adjust what is already in the file, and put in a signature - all readily available!
If you want to complete this form, be sure you enter the right details in every single blank:
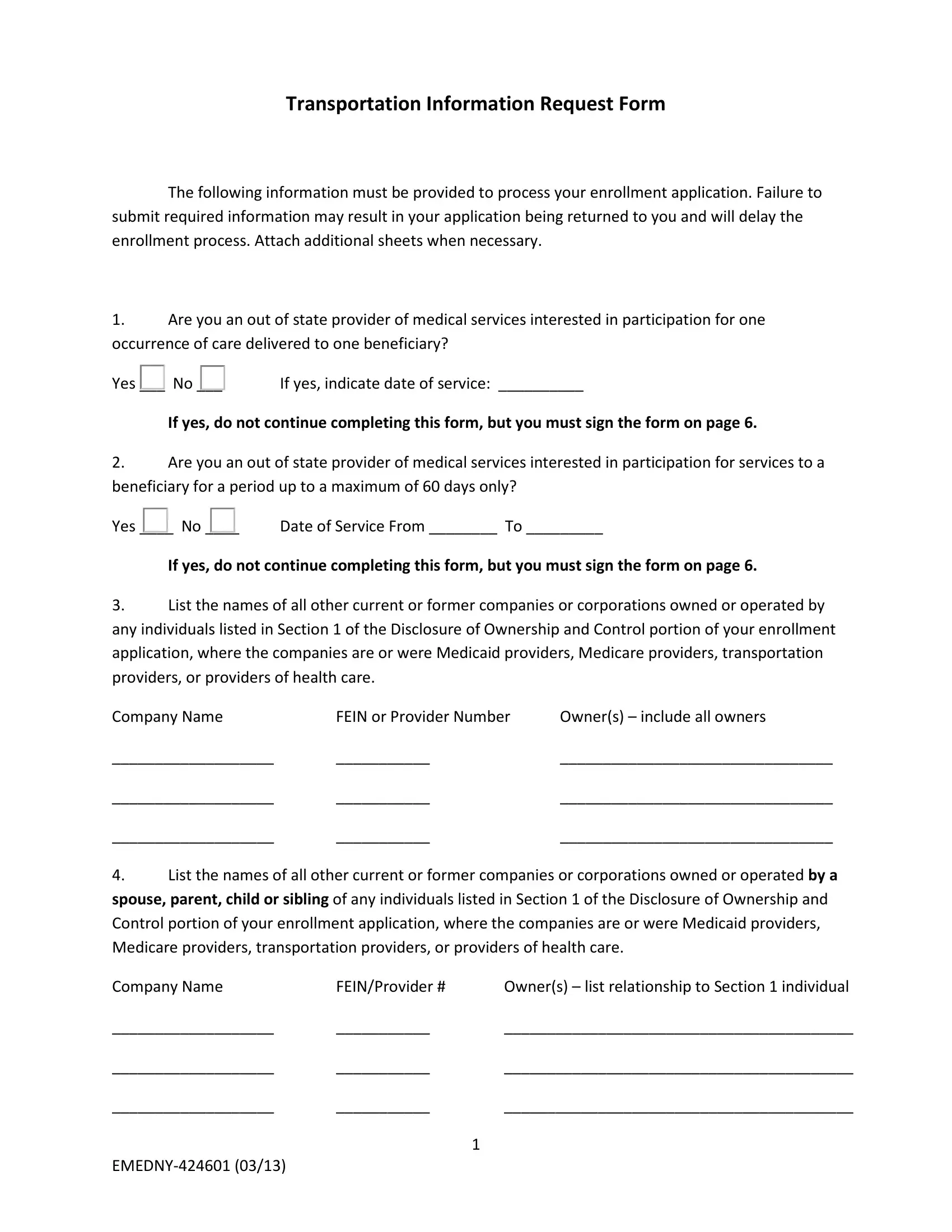
1. First, while filling out the Lic, start with the page containing next blank fields:
2. The subsequent part would be to submit the next few blank fields: List the names of all other, spouse parent child or sibling of, Control portion of your enrollment, Medicare providers transportation, Company Name, FEINProvider, Owners list relationship to, and EMEDNY.
As for Control portion of your enrollment and Company Name, be certain you review things in this current part. These could be the most important fields in this file.
3. This subsequent step should be pretty simple, Are there any other Medicaid, Yes, If yes list the provider names, List any professional licenses, Last Name First Name, Lic State, Profession, NPI or Medicaid Provider, Do any of the owners operate a, facility etc Yes, and A If yes - every one of these form fields is required to be filled in here.
4. This next section requires some additional information. Ensure you complete all the necessary fields - Name of Facility, Type of Facility, Address, Provider, Is the transportation cost, Health, Yes, C List categories of, Indicate the estimated percentage, Confined to wheelchair, Which geographic areas are you, Indicate the exact days of the, services, LiveryTaxi, and Ambulette - to proceed further in your process!
5. This last point to complete this document is critical. Make certain you fill in the required blanks, including Name of Bank, Address, Account Number, b Provide the names and social, checks against those accounts, Persons Authorized to Sign Checks, Social Security Number, and Personnel, prior to using the document. Neglecting to accomplish that might end up in an incomplete and possibly nonvalid document!
Step 3: Ensure your information is correct and just click "Done" to proceed further. Go for a free trial account with us and get immediate access to Lic - download, email, or edit from your FormsPal cabinet. We don't sell or share any information that you enter whenever working with forms at FormsPal.