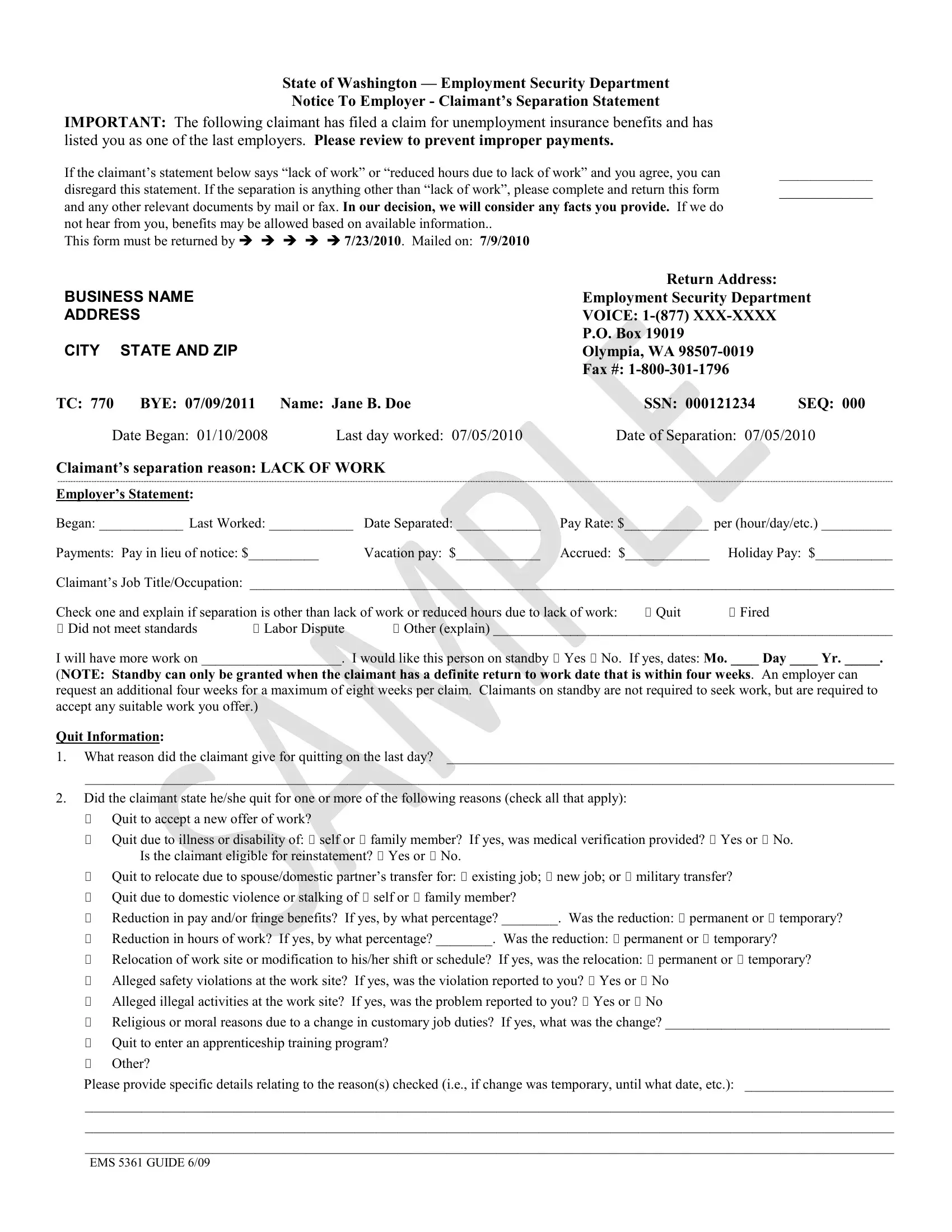
When an individual files for unemployment insurance benefits in the State of Washington, employers find themselves navigating the complexities of the Employment Security Department's procedures, particularly through the EMS 5361 form. This form, titled "Notice To Employer - Claimant's Separation Statement," serves as a critical communication bridge between employers and the Employment Security Department, ensuring that the claim for benefits is warranted and accurate. Designed to capture the circumstances surrounding an employee's departure from work, it seeks an employer's corroboration or contestation on the reasons provided by the claimant, such as "lack of work" or "reduced hours due to lack of work." Employers are urged to provide additional details if the separation reason diverges from these, thus allowing a thorough evaluation by the department. Detailed sections of the form request information about the claimant’s job title, separation conditions, and any severance details like vacation pay or pay in lieu of notice. Furthermore, it delves into specifics should the employer assert that the separation was due to resignation, discharge for cause, or other conditions that may influence the claimant's eligibility for unemployment benefits. By also addressing the possibility of standby arrangements, where a return to work date is anticipated, the form encapsulates scenarios to ensure all parties are fairly represented. Should employers overlook the directive to respond by a specified deadline, the department may proceed to adjudicate the claim with the evidence at hand, impacting the employer's experience rating and potentially the decision on the claimant’s eligibility for benefits. Thus, this document underscores the participatory role employers play in the adjudication of unemployment claims, embedding a system of checks and balances within the unemployment insurance framework.
| Question | Answer |
|---|---|
| Form Name | Form Ems 5361 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | xxxx, ems 5361, claimant, SSN |
