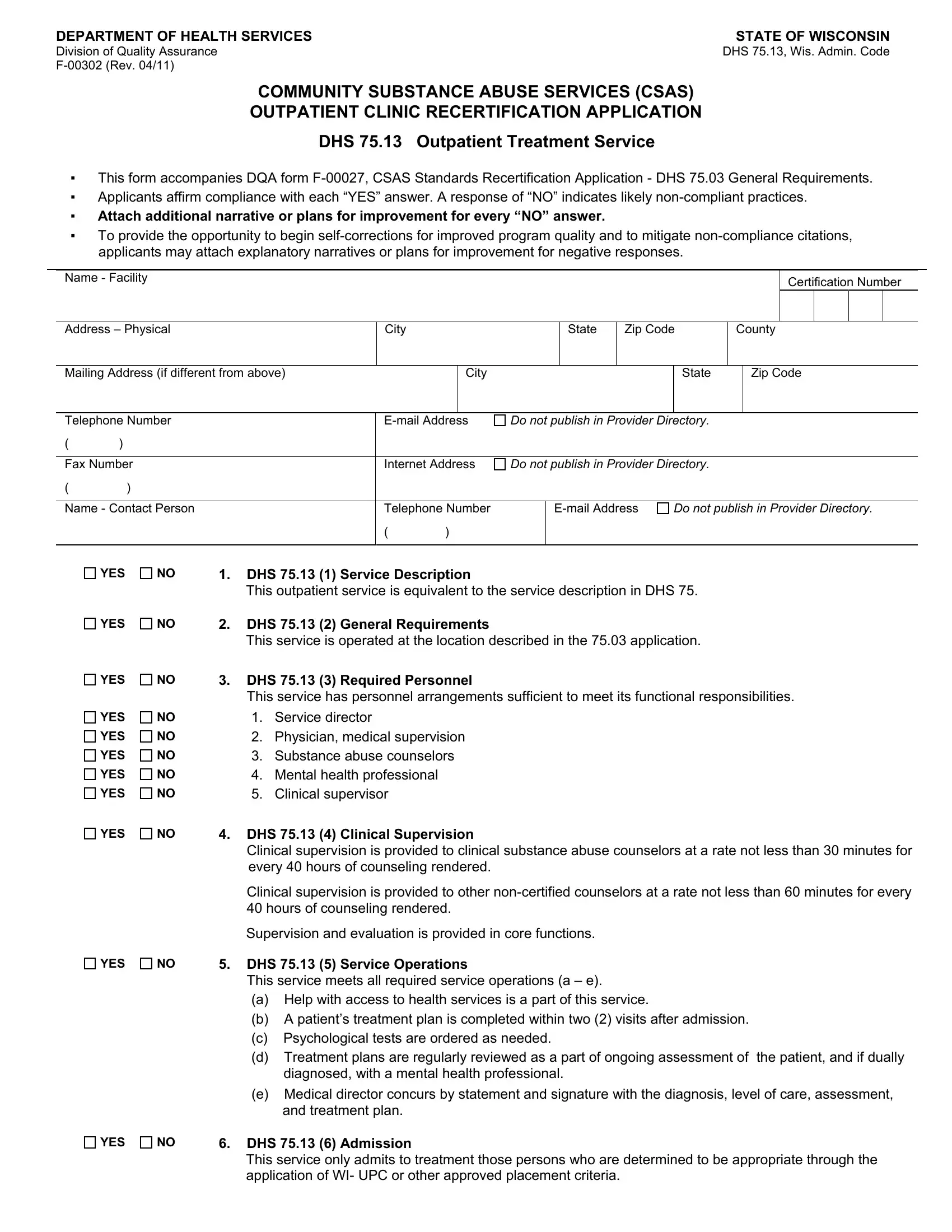
Navigating the complexities of compliance and certification in the realm of community substance abuse services becomes tangible with the understanding of the F 00302 form, issued by the Wisconsin Department of Health Services' Division of Quality Assurance. This critical document serves as an outpatient clinic recertification application, an essential step for clinics in Wisconsin that aim to continue offering outpatient treatment services under the rigorous standards set forth by DHS 75.13, Wisconsin Administrative Code. It works hand-in-glove with another form, the DQA form F-00027, highlighting the standards for recertification application and setting a comprehensive checklist to affirm compliance through affirmative responses. A unique aspect of this form is its encouragement for transparency and improvement; any "NO" response requires an attached narrative or a plan detailing the steps the facility will undertake to address non-compliance issues. This opens a pathway for clinics to not just meet the bare minimum requirements but to exceed them by continuously improving the quality of care. Moreover, it delves into specifics like personnel requirements and service operations, ensuring that each facility has the necessary arrangements to fulfill its responsibilities effectively. From helping with access to necessary health services to the intricacies of admitting patients based on established criteria, the F 00302 form encapsulates a vital process in maintaining and enhancing the quality of substance abuse treatment services within the community.
| Question | Answer |
|---|---|
| Form Name | Form F 00302 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | DHS, wisconsin dhs form f00302, explanatory, Wis |
DEPARTMENT OF HEALTH SERVICES |
STATE OF WISCONSIN |
Division of Quality Assurance |
DHS 75.13, Wis. Admin. Code |
|
COMMUNITY SUBSTANCE ABUSE SERVICES (CSAS)
OUTPATIENT CLINIC RECERTIFICATION APPLICATION
DHS 75.13 Outpatient Treatment Service
▪This form accompanies DQA form
▪Applicants affirm compliance with each “YES” answer. A response of “NO” indicates likely
▪Attach additional narrative or plans for improvement for every “NO” answer.
▪To provide the opportunity to begin
Name - Facility
Certification Number
|
|
|
|
|
|
|
|
|
|
|
|
|
Address – Physical |
City |
|
State |
Zip Code |
County |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address (if different from above) |
|
City |
|
|
|
State |
|
Zip Code |
||||
|
|
|
|
|
|
|
|
|
|
|||
Telephone Number |
Do not publish in Provider Directory. |
|
|
|
|
|
||||||
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Fax Number |
Internet Address |
Do not publish in Provider Directory. |
|
|
|
|
|
|||||
()
Name - Contact Person |
Telephone Number |
Do not publish in Provider Directory. |
()
YES |
NO |
1. |
DHS 75.13 (1) Service Description |
|
|
|
|
This outpatient service is equivalent to the service description in DHS 75. |
|
YES |
NO |
2. |
DHS 75.13 (2) General Requirements |
|
|
|
|
This service is operated at the location described in the 75.03 application. |
|
YES |
NO |
3. |
DHS 75.13 (3) Required Personnel |
|
|
|
|
This service has personnel arrangements sufficient to meet its functional responsibilities. |
|
YES |
NO |
|
1. |
Service director |
YES |
NO |
|
2. |
Physician, medical supervision |
YES |
NO |
|
3. |
Substance abuse counselors |
YES |
NO |
|
4. |
Mental health professional |
YES |
NO |
|
5. |
Clinical supervisor |
YES |
NO |
4. |
DHS 75.13 (4) Clinical Supervision |
|
|
|
|
Clinical supervision is provided to clinical substance abuse counselors at a rate not less than 30 minutes for |
|
|
|
|
every 40 hours of counseling rendered. |
|
|
|
|
Clinical supervision is provided to other |
|
|
|
|
40 hours of counseling rendered. |
|
|
|
|
Supervision and evaluation is provided in core functions. |
|
YES |
NO |
5. |
DHS 75.13 (5) Service Operations |
|
|
|
|
This service meets all required service operations (a – e). |
|
|
|
|
(a) Help with access to health services is a part of this service. |
|
|
|
|
(b) A patient’s treatment plan is completed within two (2) visits after admission. |
|
|
|
|
(c) Psychological tests are ordered as needed. |
|
|
|
|
(d) |
Treatment plans are regularly reviewed as a part of ongoing assessment of the patient, and if dually |
|
|
|
|
diagnosed, with a mental health professional. |
|
|
|
(e) Medical director concurs by statement and signature with the diagnosis, level of care, assessment, |
|
|
|
|
|
and treatment plan. |
YES |
NO |
6. |
DHS 75.13 (6) Admission |
|
|
|
|
This service only admits to treatment those persons who are determined to be appropriate through the |
|
|
|
|
application of WI- UPC or other approved placement criteria. |
|