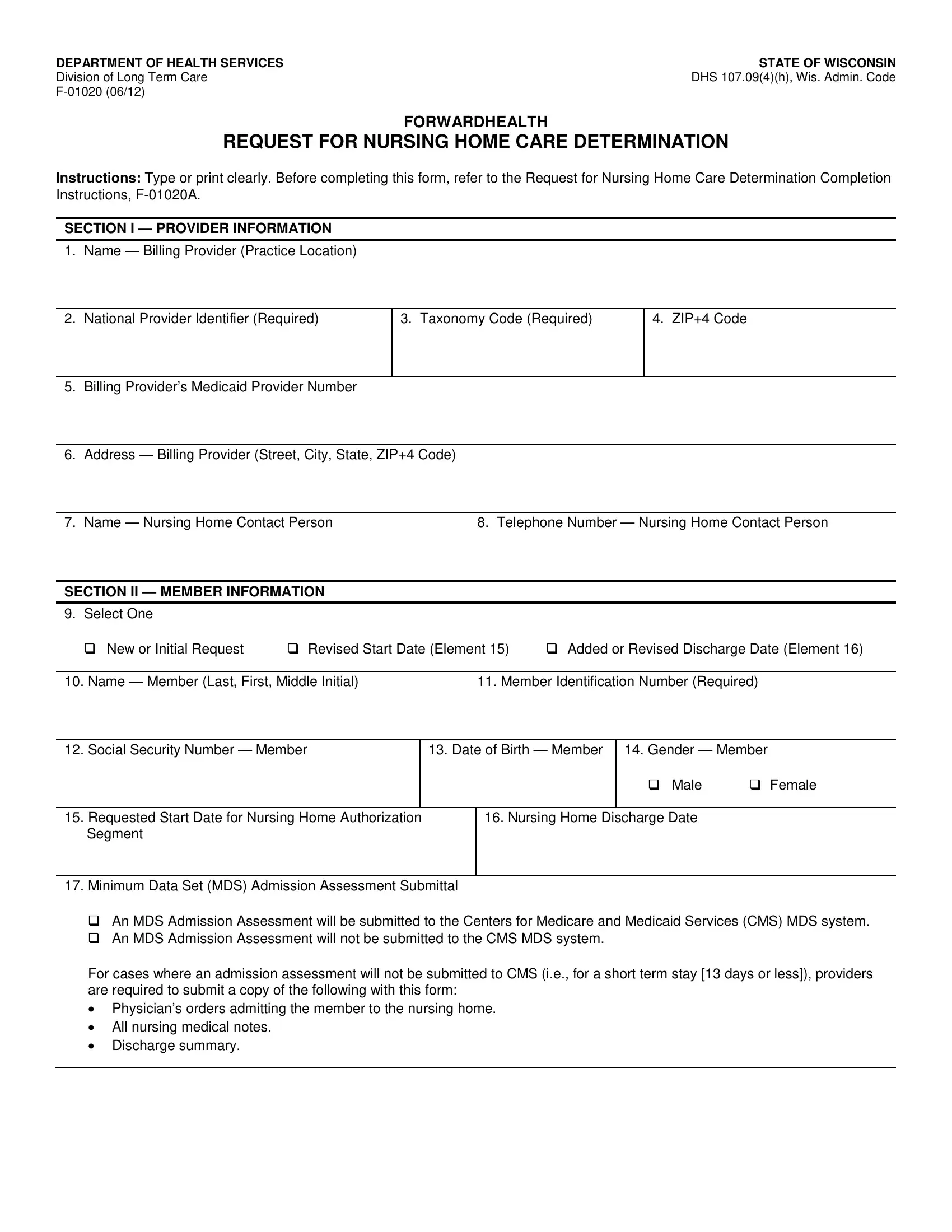
When navigating the complexities of securing nursing home care under the assistance of ForwardHealth, the F 01020 form emerges as a critical document in the State of Wisconsin. Crafted by the Department of Health Services' Division of Long Term Care, this form serves as a formal request for nursing home care determination, an essential step for both providers and members. Providers are required to furnish detailed information including their name, National Provider Identifier, and contact details, ensuring that there is a clear channel of communication from the outset. For members, the form captures vital personal information, the nature of the request—whether it's a new application or an amendment to an existing one—alongside the proposed start and, if applicable, discharge dates. A standout feature of the F 01020 form is the stipulation for submitting a Minimum Data Set (MDS) Admission Assessment to the Centers for Medicare and Medicaid Services (CMS) MDS system, emphasizing its role in streamlining the process of admissions to nursing homes. This requirement underscores the form’s comprehensive approach to facilitating accurate and efficient care determinations, reflecting a broader commitment to ensuring that individuals receive the requisite level of care tailored to their specific needs.
| Question | Answer |
|---|---|
| Form Name | Form F 01020 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Identifier, Taxonomy, Wis, DHS |
DEPARTMENT OF HEALTH SERVICES |
STATE OF WISCONSIN |
Division of Long Term Care |
DHS 107.09(4)(h), Wis. Admin. Code |
|
FORWARDHEALTH
REQUEST FOR NURSING HOME CARE DETERMINATION
INSTRUCTIONS: Type or print clearly. Before completing this form, refer to the Request for Nursing Home Care Determination Completion Instructions,
SECTION I — PROVIDER INFORMATION
1. Name — Billing Provider (Practice Location)
2. National Provider Identifier (Required)
3. Taxonomy Code (Required)
4. ZIP+4 Code
5.Billing Provider’s Medicaid Provider Number
6.Address — Billing Provider (Street, City, State, ZIP+4 Code)
7. Name — Nursing Home Contact Person
8. Telephone Number — Nursing Home Contact Person
SECTION II — MEMBER INFORMATION
9. Select One
New or Initial Request |
Revised Start Date (Element 15) |
Added or Revised Discharge Date (Element 16) |
10. Name — Member (Last, First, Middle Initial)
11. Member Identification Number (Required)
12. Social Security Number — Member
13. Date of Birth — Member
14. Gender — Member
Male |
Female |
15.Requested Start Date for Nursing Home Authorization Segment
16. Nursing Home Discharge Date
17.Minimum Data Set (MDS) Admission Assessment Submittal
An MDS Admission Assessment will be submitted to the Centers for Medicare and Medicaid Services (CMS) MDS system.
An MDS Admission Assessment will not be submitted to the CMS MDS system.
For cases where an admission assessment will not be submitted to CMS (i.e., for a short term stay [13 days or less]), providers are required to submit a copy of the following with this form:
•Physician’s orders admitting the member to the nursing home.
•All nursing medical notes.
•Discharge summary.