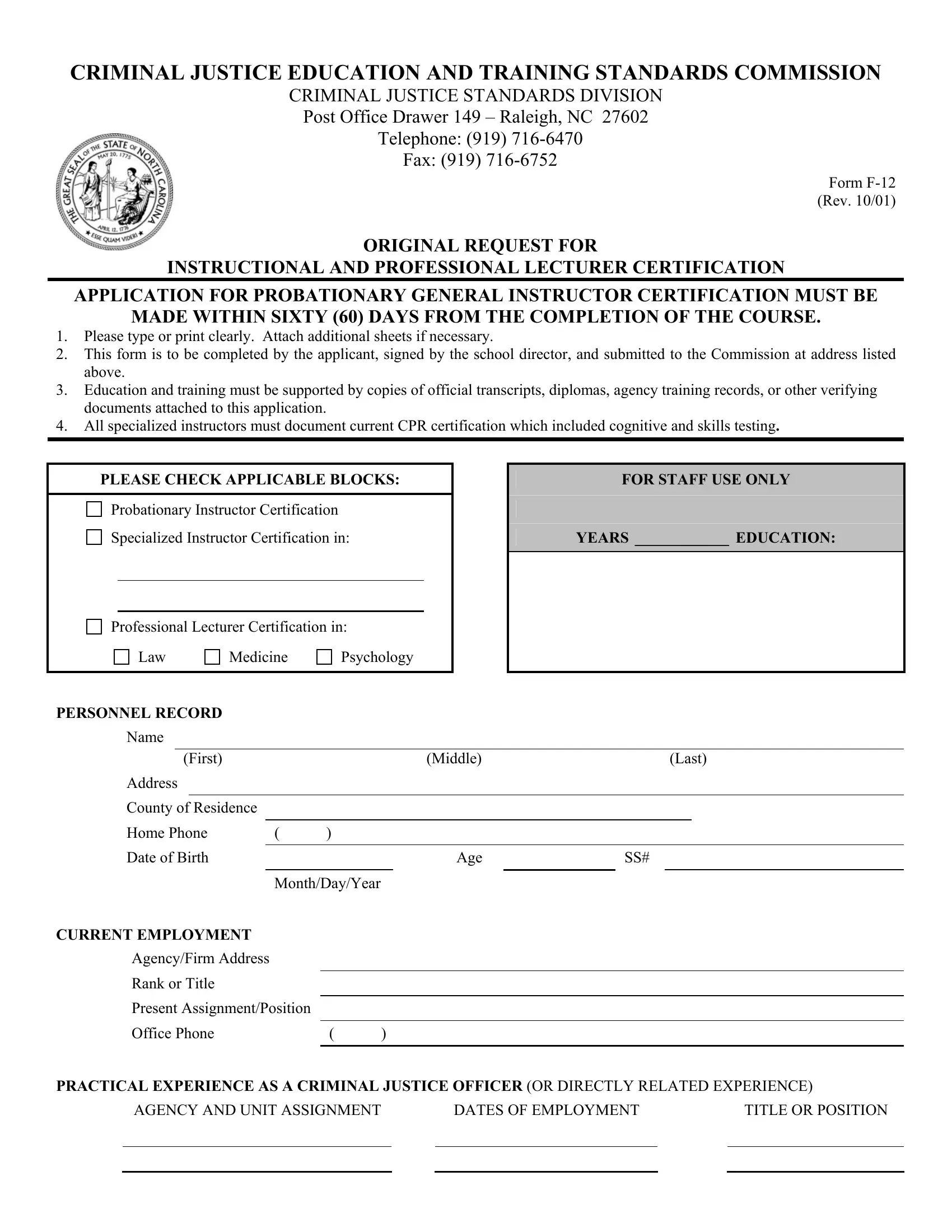
Embarking on a career in criminal justice education and training requires thorough preparation and compliance with specific standards. Among the crucial steps for professionals aspiring to enhance their teaching credentials within this field is the completion of the Form F-12. Managed by the Criminal Justice Education and Training Standards Commission, this form is a requisite for individuals seeking probationary general instructor certification, specialized instructor certification in law, medicine, psychology, or professional lecturer certification. The application process underscores the significance of timely submission—specifically within sixty days following the course completion. Additionally, it mandates the provision of detailed educational and practical experience documentation, along with verification of CPR certification for specialized instructors. This process not only evaluates the applicant’s qualifications but also ensures adherence to high standards of instructional quality and ethical conduct. The requirement for a recommendation from a certified school director further validates the applicant’s moral character and capability to train future criminal justice personnel effectively. By navigating through these meticulously designed steps, applicants are better positioned to contribute significantly to the field of criminal justice education and training.
| Question | Answer |
|---|---|
| Form Name | Form F 12 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | f12 form, Raleigh, F-12, form f12 |
