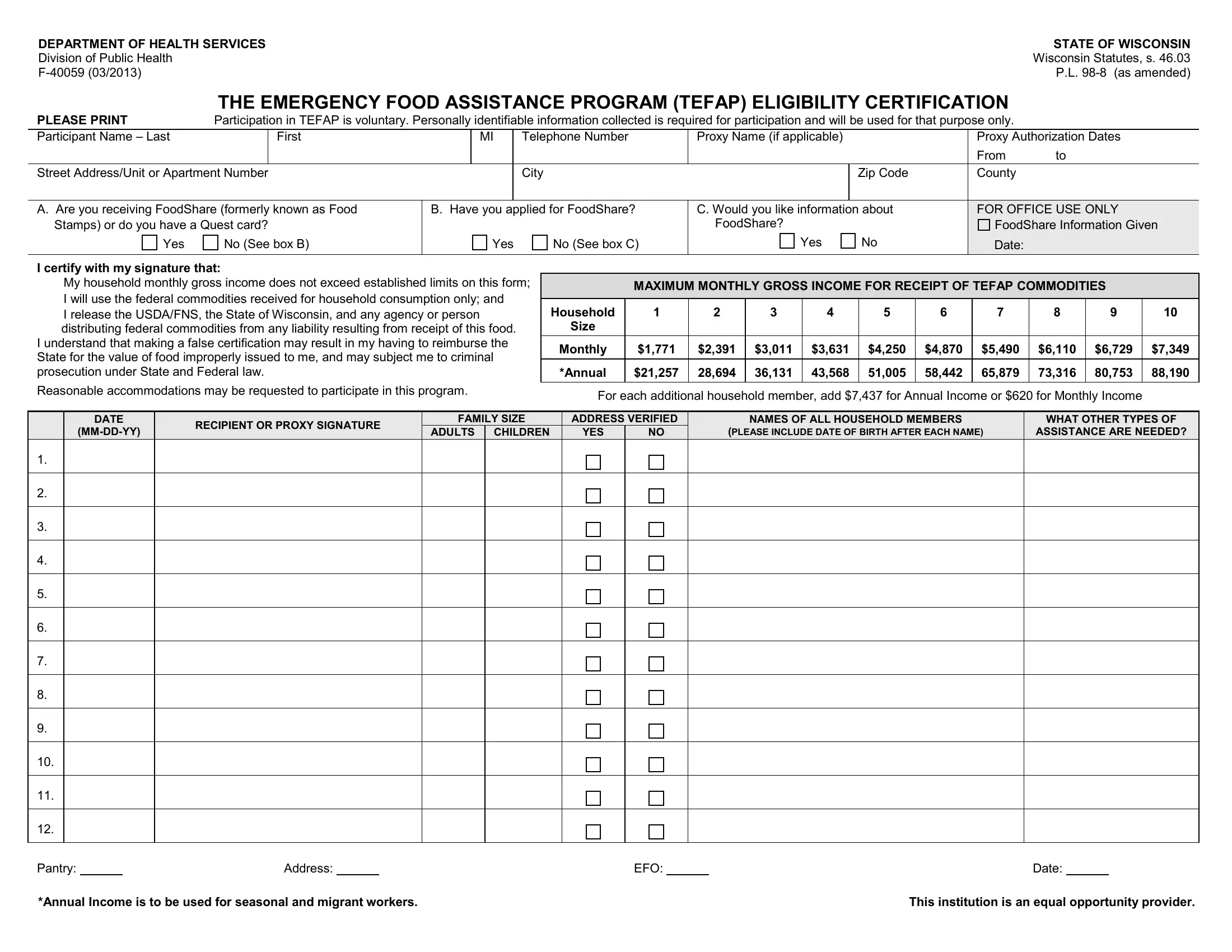
In the realm of assistance programs within the United States, the Emergency Food Assistance Program (TEFAP) stands as a crucial component in the fight against hunger, providing eligible individuals and families with the necessary resources to secure food. The form F-40059, underpinning this program in the state of Wisconsin, operates as a tool for certifying the eligibility of applicants seeking aid. Rooted in the Wisconsin Statutes, s. 46.03, and amended by public law P.L. 98-8, this form encompasses a breadth of information, from personal identification to income verification, aiming to streamline the participation process. Prospective participants are required to divulge comprehensive details such as household income, familial size, and if they are currently receiving or have applied for FoodShare benefits, previously known as Food Stamps. It mandates the applicant's acknowledgment concerning the use of aid—ensuring that the resources provided are destined solely for household consumption—and clearly outlines the repercussions of false certification. Moreover, it underscores the program's dedication to inclusivity and accessibility by making provisions for reasonable accommodations. Through this form, the intricate balance of ensuring aid reaches those in genuine need while safeguarding against misuse of resources is navigated, reflecting a broader commitment to both accountability and support within public aid initiatives.
| Question | Answer |
|---|---|
| Form Name | Form F 40059 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | F40059 tefap eligibility form wisconsin |
DEPARTMENT OF HEALTH SERVICES |
STATE OF WISCONSIN |
Division of Public Health |
Wisconsin Statutes, s. 46.03 |
P.L. |
THE EMERGENCY FOOD ASSISTANCE PROGRAM (TEFAP) ELIGIBILITY CERTIFICATION
PLEASE PRINT |
Participation in TEFAP is voluntary. Personally identifiable information collected is required for participation and will be used for that purpose only. |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
Participant Name – Last |
|
First |
|
MI |
|
Telephone Number |
Proxy Name (if applicable) |
|
Proxy Authorization Dates |
|
|
|
|
|
|
|
|
|
|
From |
to |
Street Address/Unit or Apartment Number |
|
|
|
City |
|
Zip Code |
County |
|
||
|
|
|
|
|
|
|||||
A. Are you receiving FoodShare (formerly known as Food |
B. Have you applied for FoodShare? |
C. Would you like information about |
FOR OFFICE USE ONLY |
|||||||
Stamps) or do you have a Quest card? |
|
|
|
|
FoodShare? |
|
FoodShare Information Given |
|||
Yes |
No (See box B) |
|
Yes |
No (See box C) |
Yes |
No |
Date: |
|
||
|
|
|
|
|
|
|
|
|
|
|
I certify with my signature that:
My household monthly gross income does not exceed established limits on this form;
I will use the federal commodities received for household consumption only; and
I release the USDA/FNS, the State of Wisconsin, and any agency or person distributing federal commodities from any liability resulting from receipt of this food.
I understand that making a false certification may result in my having to reimburse the State for the value of food improperly issued to me, and may subject me to criminal prosecution under State and Federal law.
Reasonable accommodations may be requested to participate in this program.
MAXIMUM MONTHLY GROSS INCOME FOR RECEIPT OF TEFAP COMMODITIES
|
|
|
|
|
|
|
|
|
|
|
Household |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
Size |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Monthly |
$1,771 |
$2,391 |
$3,011 |
$3,631 |
$4,250 |
$4,870 |
$5,490 |
$6,110 |
$6,729 |
$7,349 |
|
|
|
|
|
|
|
|
|
|
|
*Annual |
$21,257 |
28,694 |
36,131 |
43,568 |
51,005 |
58,442 |
65,879 |
73,316 |
80,753 |
88,190 |
|
|
|
|
|
|
|
|
|
|
|
For each additional household member, add $7,437 for Annual Income or $620 for Monthly Income
DATE |
RECIPIENT OR PROXY SIGNATURE |
FAMILY SIZE |
ADDRESS VERIFIED |
NAMES OF ALL HOUSEHOLD MEMBERS |
WHAT OTHER TYPES OF |
|||
ADULTS |
CHILDREN |
YES |
NO |
(PLEASE INCLUDE DATE OF BIRTH AFTER EACH NAME) |
ASSISTANCE ARE NEEDED? |
|||
|
||||||||
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Pantry: |
|
Address: |
|
EFO: |
|
Date: |
*Annual Income is to be used for seasonal and migrant workers. |
This institution is an equal opportunity provider. |