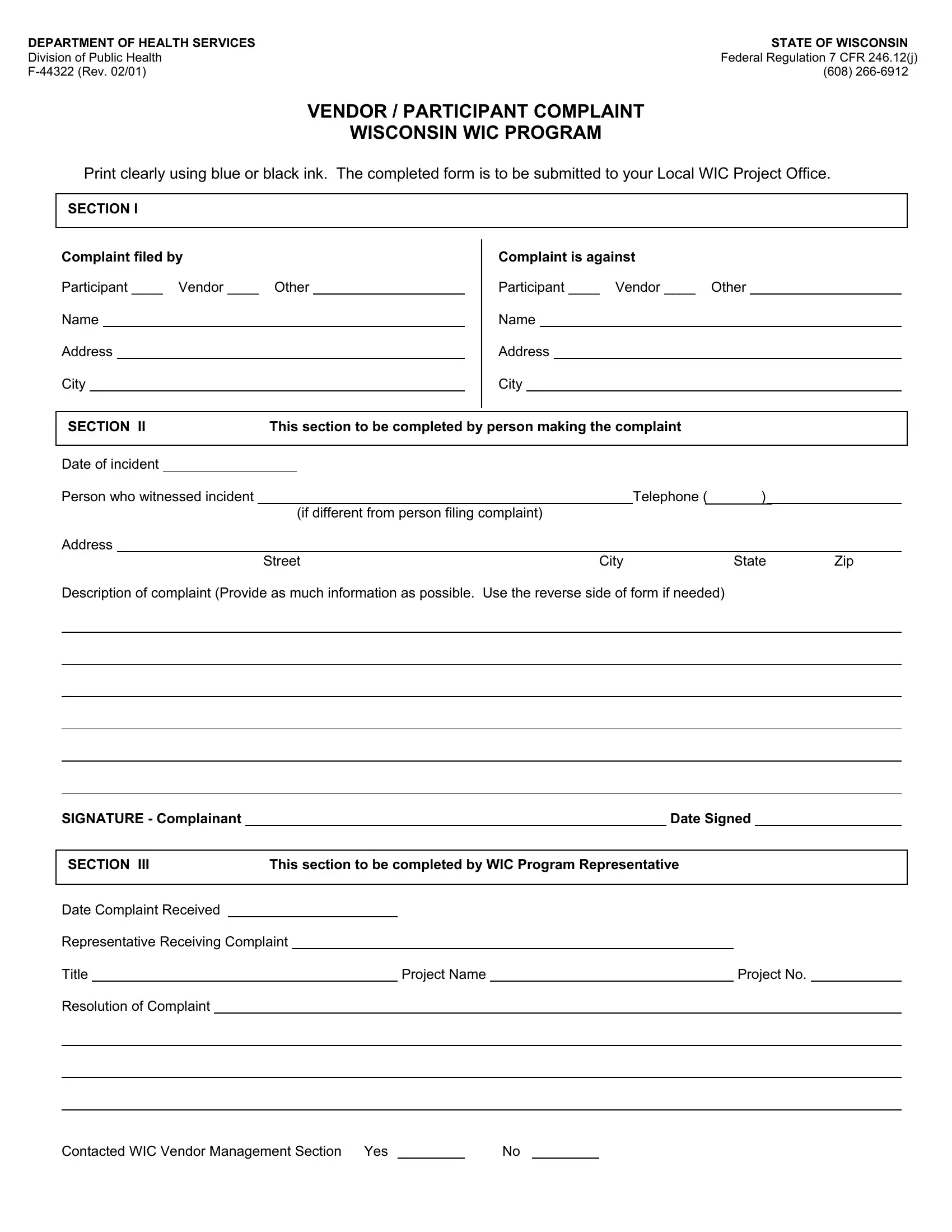
Access to fair and effective complaint processes is crucial for maintaining trust and accountability in any public program, and the Wisconsin WIC (Women, Infants, and Children) Program is no exception. The F-44322 form plays a pivotal role in this process by offering participants and vendors a structured way to report their grievances. Crafted under the guidelines of Federal Regulation 7 CFR 246.12(j) and revised in February 2001, this document ensures that every voice can be heard and every concern addressed in a systematic manner. Whether a complaint is filed by a participant, a vendor, or an external party, the form guides the complainant through providing detailed information about the incident, including the date, the parties involved, and a comprehensive description of the complaint. This meticulous approach ensures that the WIC Program representatives have all the necessary information to make informed decisions and address issues effectively. The resolution process also includes steps for the program representative, promoting transparency and accountability at every stage. Designed to be filled out with blue or black ink, this form is a testament to the Wisconsin WIC Program's commitment to upholding the highest standards of service and care for its participants and stakeholders.
| Question | Answer |
|---|---|
| Form Name | Form F 44322 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | F44322 wisconsin wic vendor form |
DEPARTMENT OF HEALTH SERVICES |
STATE OF WISCONSIN |
Division of Public Health |
Federal Regulation 7 CFR 246.12(j) |
(608) |
VENDOR / PARTICIPANT COMPLAINT
WISCONSIN WIC PROGRAM
Print clearly using blue or black ink. The completed form is to be submitted to your Local WIC Project Office.
SECTION I
Complaint filed by
Participant ____ Vendor ____ Other
Name
Address
City
Complaint is against
Participant ____ Vendor ____ Other
Name
Address
City
SECTION II |
This section to be completed by person making the complaint |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
||
Date of incident |
|
|
|
|
|
|
|
|
|
|
Person who witnessed incident |
|
|
|
Telephone ( |
) |
|
|
|||
|
|
|
(if different from person filing complaint) |
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
||
|
|
|
Street |
City |
State |
Zip |
|
|||
Description of complaint (Provide as much information as possible. Use the reverse side of form if needed)
SIGNATURE - Complainant |
|
Date Signed |
|
|
|
|
|
|
|
SECTION III |
This section to be completed by WIC Program Representative |
|||
|
|
|
|
|
Date Complaint Received |
|
|
|
|
|
|||
Representative Receiving Complaint |
|
|
|
|
|
|||
Title |
|
Project Name |
|
Project No. |
|
|||
Resolution of Complaint |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Contacted WIC Vendor Management Section Yes |
|
No |