

Using PDF documents online is very easy using our PDF editor. Anyone can fill out form f7 here effortlessly. Our tool is continually developing to give the best user experience attainable, and that is thanks to our dedication to continuous improvement and listening closely to customer opinions. Here's what you'd want to do to get going:
Step 1: Click the orange "Get Form" button above. It's going to open our tool so that you could begin completing your form.
Step 2: The editor will let you customize PDF files in a range of ways. Enhance it with customized text, correct what's already in the document, and add a signature - all within several mouse clicks!
This PDF form will require specific info to be entered, so be certain to take whatever time to enter what's required:
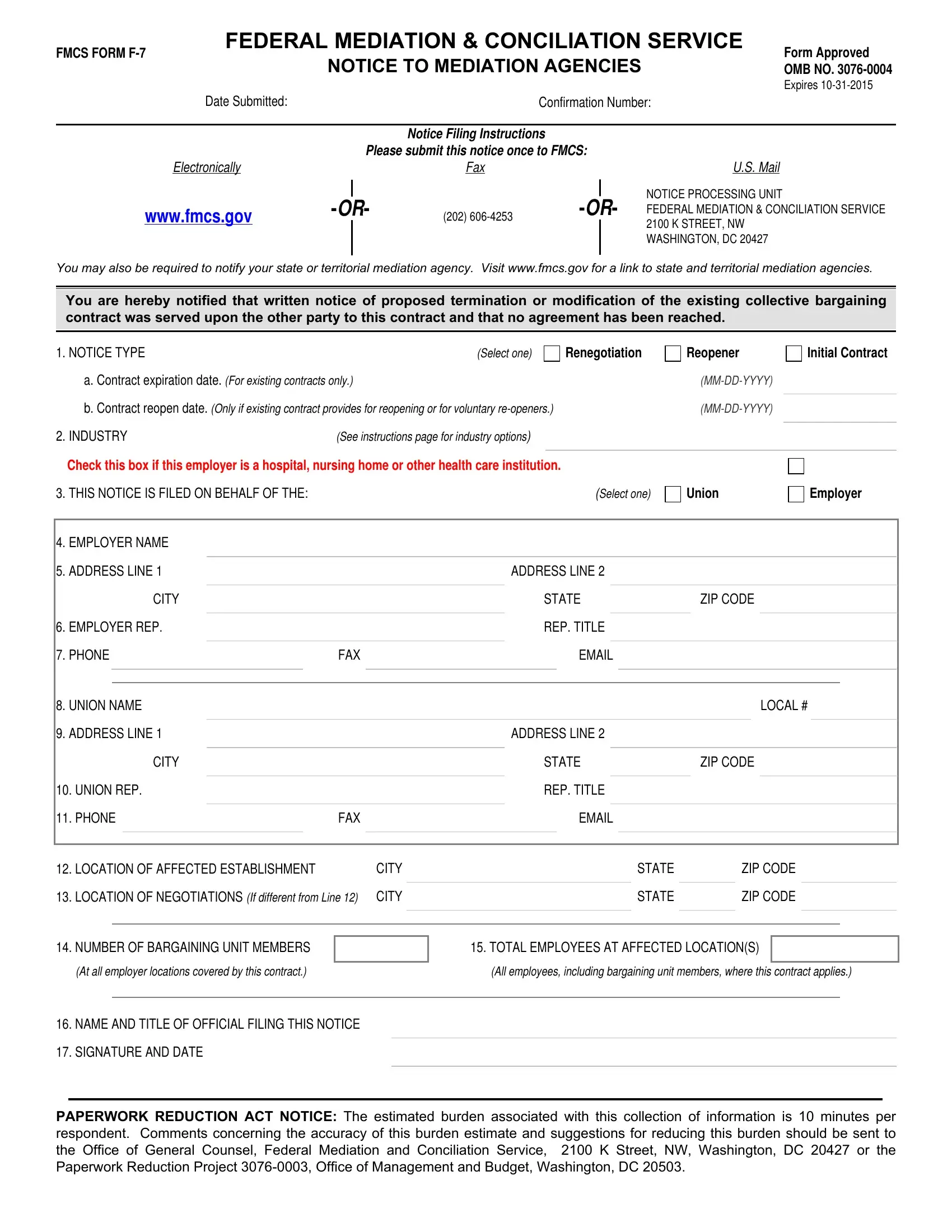
1. To start with, once completing the form f7, start out with the area that has the following blank fields:
2. The subsequent stage is usually to submit these fields: EMPLOYER NAME, ADDRESS LINE, CITY, EMPLOYER REP, PHONE, FAX, UNION NAME, ADDRESS LINE, CITY, UNION REP, PHONE, FAX, ADDRESS LINE, STATE, and REP TITLE.
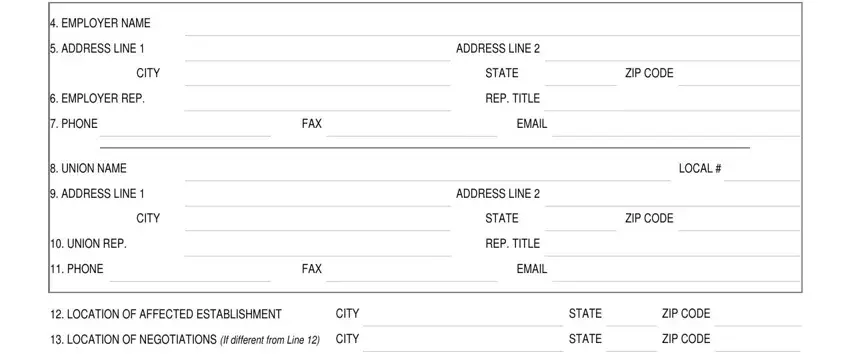
In terms of EMPLOYER NAME and UNION NAME, ensure that you do everything right in this section. The two of these are thought to be the most significant fields in the file.
3. This next section focuses on NUMBER OF BARGAINING UNIT MEMBERS, TOTAL EMPLOYEES AT AFFECTED, At all employer locations covered, All employees including bargaining, NAME AND TITLE OF OFFICIAL FILING, SIGNATURE AND DATE, and PAPERWORK REDUCTION ACT NOTICE The - fill out all these empty form fields.
Step 3: Confirm that your information is correct and then simply click "Done" to complete the project. Find your form f7 when you sign up for a 7-day free trial. Instantly view the pdf file from your FormsPal account, together with any edits and adjustments conveniently preserved! FormsPal guarantees your information confidentiality via a protected system that never records or shares any kind of personal data provided. Rest assured knowing your docs are kept protected any time you use our editor!