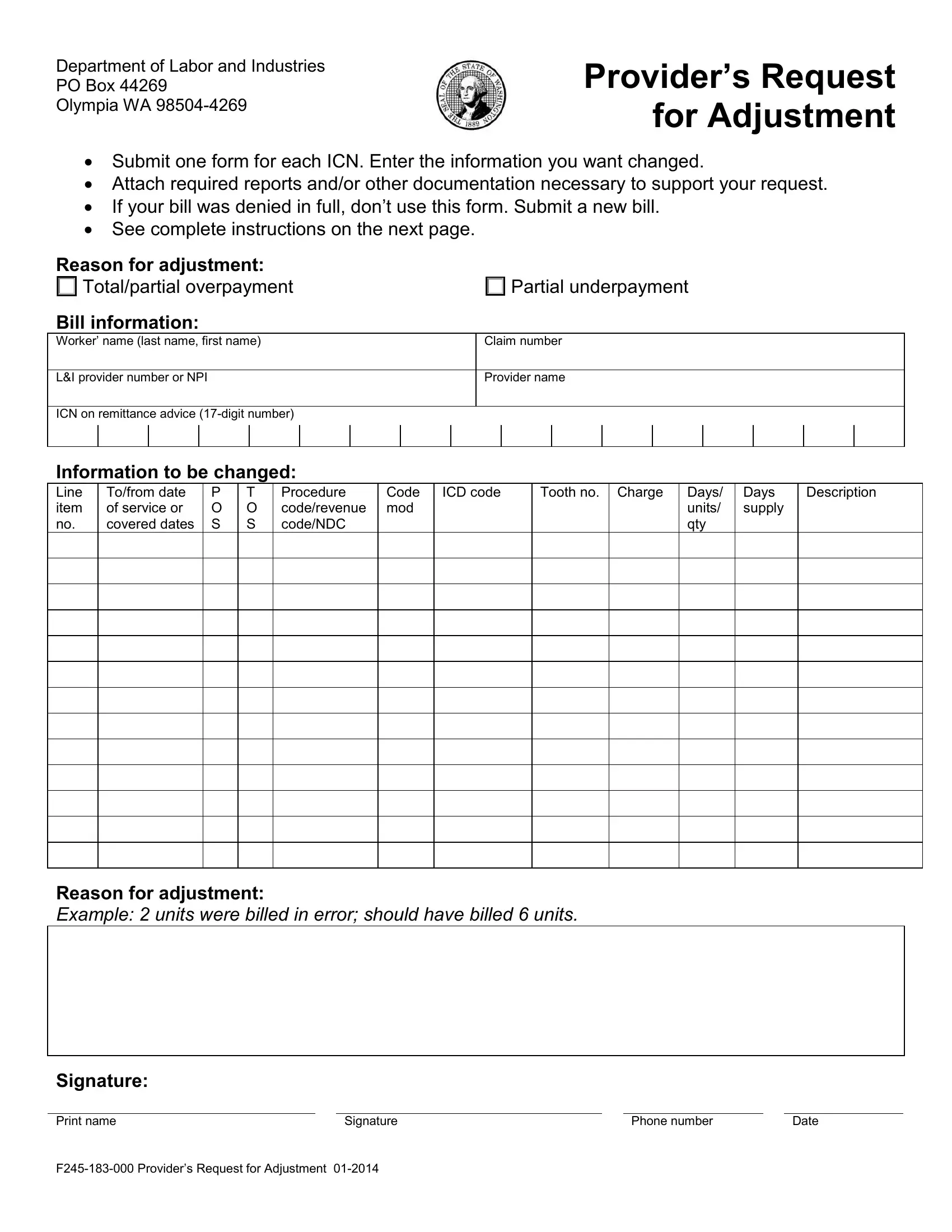
In the complex realm of healthcare billing, especially when dealing with workers' compensation claims, navigating the process of adjusting a bill can be challenging. This is where the F245 183 000 form, officially known as the Provider’s Request for Adjustment, comes into play. It serves as a crucial tool for healthcare providers to request adjustments on bills submitted to the Department of Labor and Industries. Whether due to a full or partial overpayment or underpayment, this form allows for the correction of bill details including the worker's name, claim number, provider number, and specific information about the items or services billed, such as dates of service, types of service (TOS), procedure codes, and charges. The form requires detailed justification for the adjustment, supported by attaching necessary documentation. It's important to note that this form should not be used in situations where the bill was denied in full; instead, a new bill should be submitted. The form not only facilitates the adjustment process but also demonstrates the Department's efforts to streamline healthcare billing corrections, ensuring providers are fairly compensated for their services and that errors can be rectified promptly. Understanding and correctly completing the F245 183 000 form is integral for healthcare providers who navigate the intricacies of workers' compensation claims.
| Question | Answer |
|---|---|
| Form Name | Form F245 183 000 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | F245 183 000 f245 183 000 form |
