
You can fill in Ostomy instantly in our online PDF tool. Our team is continuously endeavoring to improve the tool and make it much easier for clients with its extensive features. Enjoy an ever-evolving experience now! This is what you'll have to do to start:
Step 1: Press the "Get Form" button at the top of this page to open our PDF editor.
Step 2: When you launch the tool, there'll be the document made ready to be completed. In addition to filling out various blanks, you may also do other things with the file, that is putting on custom words, changing the initial textual content, adding images, putting your signature on the document, and much more.
This PDF doc will need specific details; in order to guarantee accuracy, please be sure to take into account the subsequent steps:
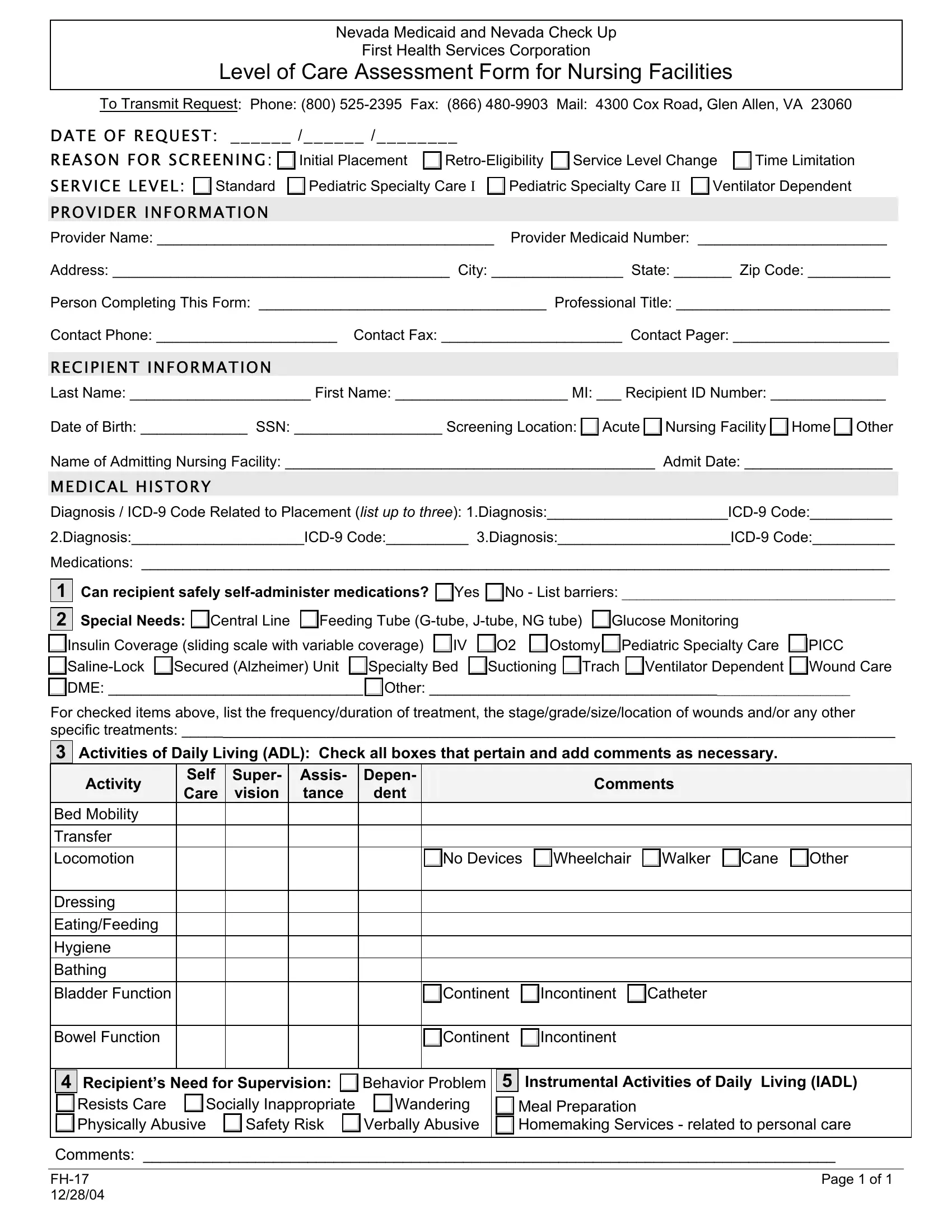
1. Begin completing your Ostomy with a number of essential blank fields. Get all of the necessary information and be sure not a single thing omitted!
2. Soon after completing this step, go to the subsequent part and enter the essential details in these fields - DiagnosisICD Code DiagnosisICD Code, Medications, Can recipient safely, Special Needs Central Line, Insulin Coverage sliding scale, IV O, Ostomy Pediatric Specialty Care, SalineLock Secured Alzheimer Unit, DME Other, For checked items above list the, Self Care, Super vision, Assis tance, Depen dent, and Comments.
3. The next step is simple - fill in all the blanks in Bowel Function, Continent, Incontinent, Recipients Need for Supervision, Behavior Problem, Instrumental Activities of Daily, Resists Care Physically Abusive, Socially Inappropriate, Wandering, Safety Risk, Verbally Abusive, Meal Preparation Homemaking, Comments, and Page of to complete this segment.
People generally get some things wrong while filling in Verbally Abusive in this section. Be sure you revise whatever you type in right here.
Step 3: Prior to finishing this form, it's a good idea to ensure that blanks have been filled in the right way. The moment you are satisfied with it, click on “Done." Right after getting a7-day free trial account at FormsPal, you'll be able to download Ostomy or send it via email right off. The PDF document will also be available through your personal account page with all of your adjustments. We do not share or sell any information you enter whenever filling out documents at our site.