
fr 309 can be filled out easily. Simply try FormsPal PDF editing tool to finish the job fast. In order to make our editor better and easier to utilize, we consistently develop new features, taking into account suggestions coming from our users. With a few basic steps, it is possible to begin your PDF journey:
Step 1: Open the PDF file in our editor by hitting the "Get Form Button" above on this page.
Step 2: With this advanced PDF file editor, you can do more than just fill in blank form fields. Try all the features and make your forms seem perfect with custom text put in, or modify the original input to excellence - all that accompanied by the capability to incorporate your own images and sign the PDF off.
It will be straightforward to finish the document using out detailed guide! Here's what you have to do:
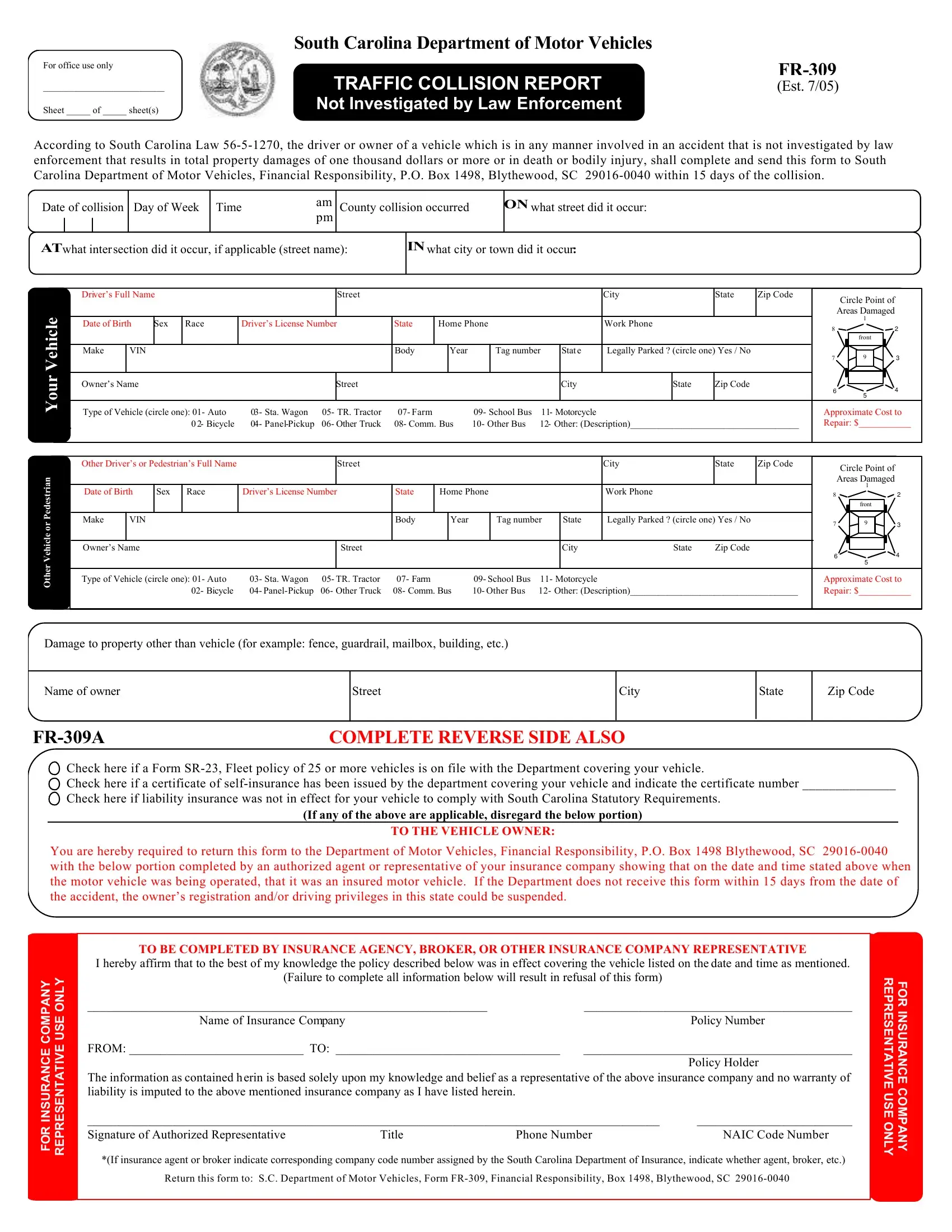
1. To start off, once filling in the fr 309, start out with the area with the next fields:
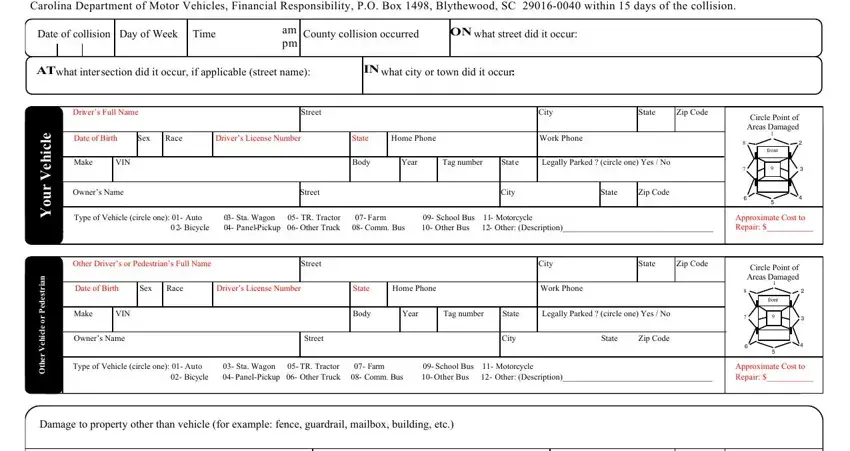
2. Given that the previous segment is done, you're ready add the necessary specifics in Damage to property other than, Name of owner, FRA FR, Street, City, State, Zip Code, COMPLETE REVERSE SIDE ALSO, Check here if a Form SR Fleet, If any of the above are applicable, TO THE VEHICLE OWNER, You are hereby required to return, TO BE COMPLETED BY INSURANCE, I hereby affirm that to the best, and Y N A P M O C E C N A R U S N so you're able to move forward further.
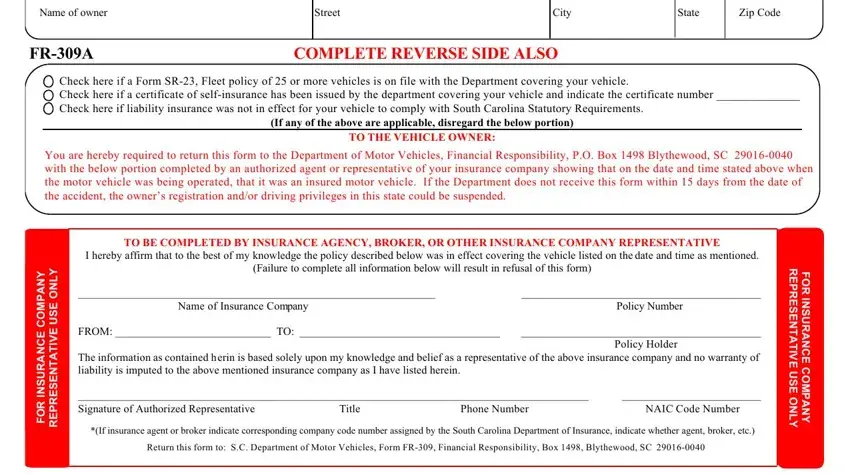
As to Check here if a Form SR Fleet and Damage to property other than, make sure you get them right here. The two of these are viewed as the most significant ones in this page.
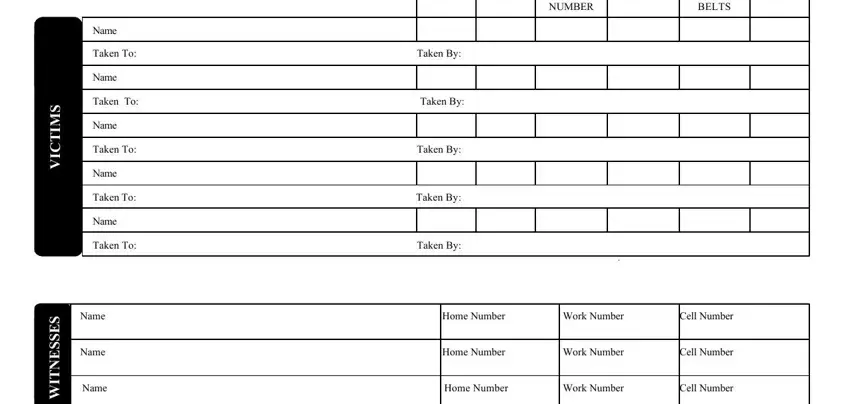
3. Completing AGE, VEHICLE NUMBER, SAFETY BELTS, Name, Taken To Taken By, Name, Taken To Taken By, Name, Taken To Taken By, Name Taken To Taken By, Name Taken To Taken By, Name Home Number, Name Home Number, Name Home Number, and Work Number is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
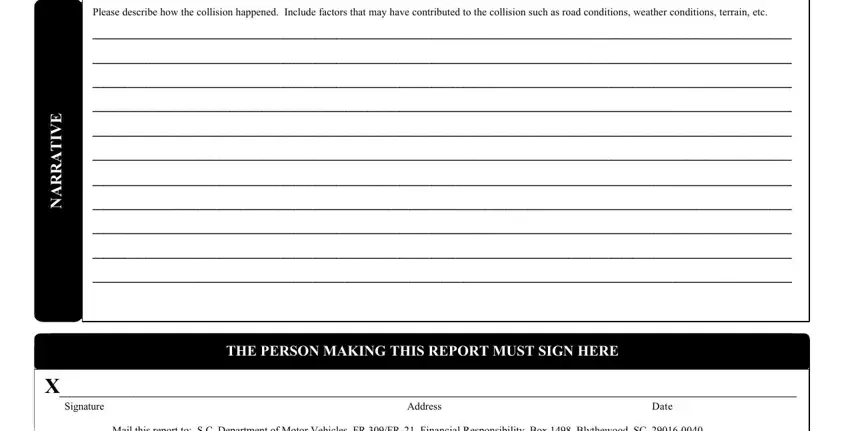
4. This next section requires some additional information. Ensure you complete all the necessary fields - Please describe how the collision, THE PERSON MAKING THIS REPORT MUST, E V I T A R R A N, Signature Address, Mail this report to SC Department, and Date - to proceed further in your process!
Step 3: Immediately after rereading your completed blanks, click "Done" and you're done and dusted! Right after getting afree trial account at FormsPal, you'll be able to download fr 309 or send it through email right off. The PDF file will also be readily available through your personal account page with your every modification. FormsPal is invested in the privacy of all our users; we make sure all personal information entered into our editor is kept protected.