
Working with PDF documents online is definitely simple with our PDF editor. You can fill in Form Ga 72000 here effortlessly. FormsPal team is aimed at making sure you have the best possible experience with our tool by continuously presenting new features and upgrades. With these improvements, working with our tool becomes better than ever before! By taking a few basic steps, it is possible to start your PDF journey:
Step 1: First of all, open the tool by pressing the "Get Form Button" in the top section of this page.
Step 2: The tool gives you the capability to customize nearly all PDF forms in various ways. Modify it by adding your own text, correct existing content, and put in a signature - all within several mouse clicks!
Completing this document will require focus on details. Make certain all required areas are filled in accurately.
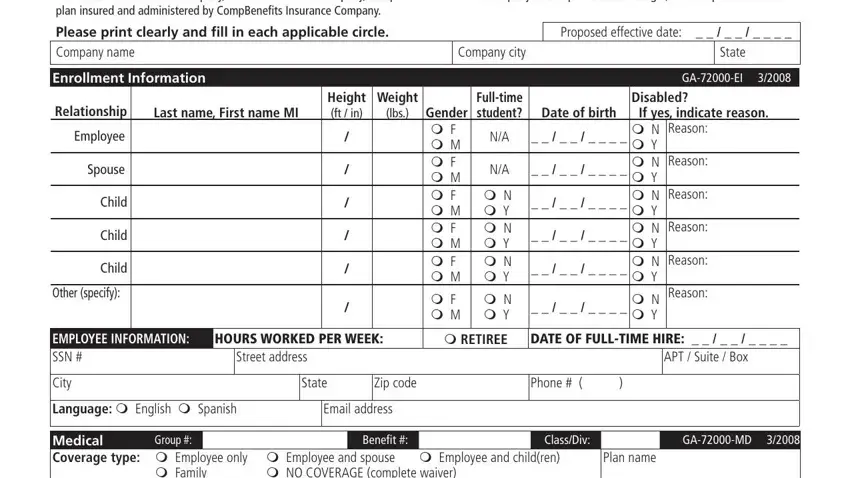
1. The Form Ga 72000 will require certain details to be entered. Be sure that the following fields are complete:
2. After filling in the previous section, go to the next step and complete all required details in all these fields - Medical Coverage type m Employee, m NO COVERAGE complete waiver, m Family, Prior coverage type m Employee, m Employee and spouse, Effective date, Term date, Other medical coverage in effect, Other coverage type m Employee, m Employee and spouse, Term date, Medicare coverage Employee, Medicare ID, Medicare ID, and Effective date Effective.
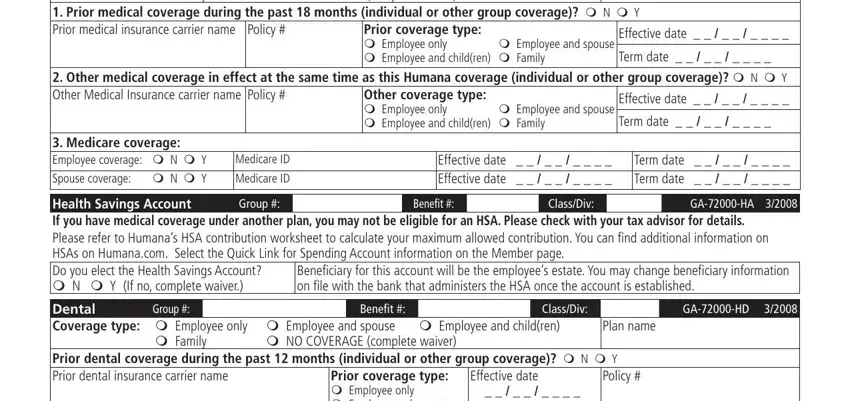
3. Completing Prior orthodontia coverage in the, Prior carrier phone, Reorder GAHH, Prior coverage type m Employee, and Effective date Term date is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Concerning Effective date Term date and Prior carrier phone, be sure that you review things in this section. Those two are certainly the most significant fields in this file.
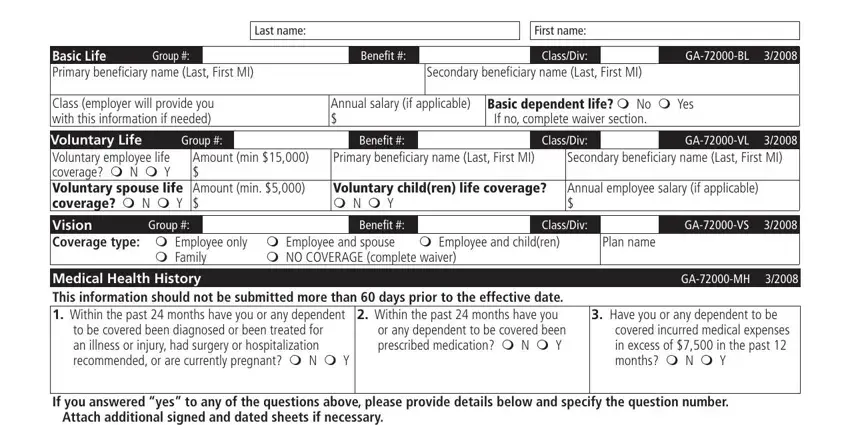
4. The form's fourth part comes with the next few blanks to focus on: Basic Life Primary beneiciary name, Group, Benefit, Last name, First name, ClassDiv, GABL, Secondary beneiciary name Last, Class employer will provide you, Annual salary if applicable, Basic dependent life m No m Yes If, Group, Voluntary Life Voluntary employee, Amount min Amount min, and Benefit.
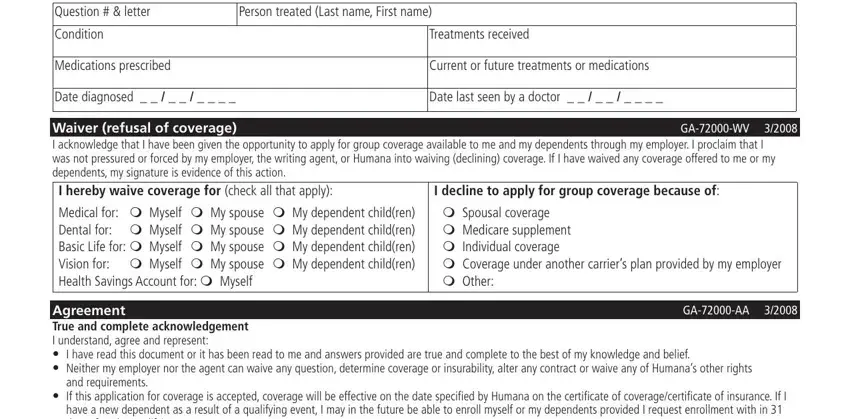
5. To wrap up your form, the particular segment features some additional blanks. Completing If you answered yes to any of the, Person treated Last name First name, Condition, Medications prescribed, Treatments received, Current or future treatments or, Date diagnosed, Date last seen by a doctor, Waiver refusal of coverage I, m Spousal coverage m Medicare, I decline to apply for group, GAWV, GAAA, Agreement True and complete, and I have read this document or it should finalize everything and you will be done in a blink!
Step 3: Once you have glanced through the information you given, press "Done" to conclude your form. Try a 7-day free trial option with us and get instant access to Form Ga 72000 - download or modify from your FormsPal account page. FormsPal offers risk-free document tools devoid of data recording or any sort of sharing. Feel safe knowing that your details are secure with us!