
If you want to fill out california application order authorizing, you don't need to install any applications - simply try using our PDF tool. FormsPal professional team is relentlessly endeavoring to enhance the editor and make it even faster for clients with its extensive functions. Enjoy an ever-evolving experience now! Here is what you will have to do to get started:
Step 1: Click the "Get Form" button at the top of this page to get into our PDF editor.
Step 2: The tool enables you to work with PDF forms in many different ways. Modify it by writing personalized text, correct original content, and put in a signature - all when it's needed!
It is an easy task to complete the form with our helpful guide! This is what you need to do:
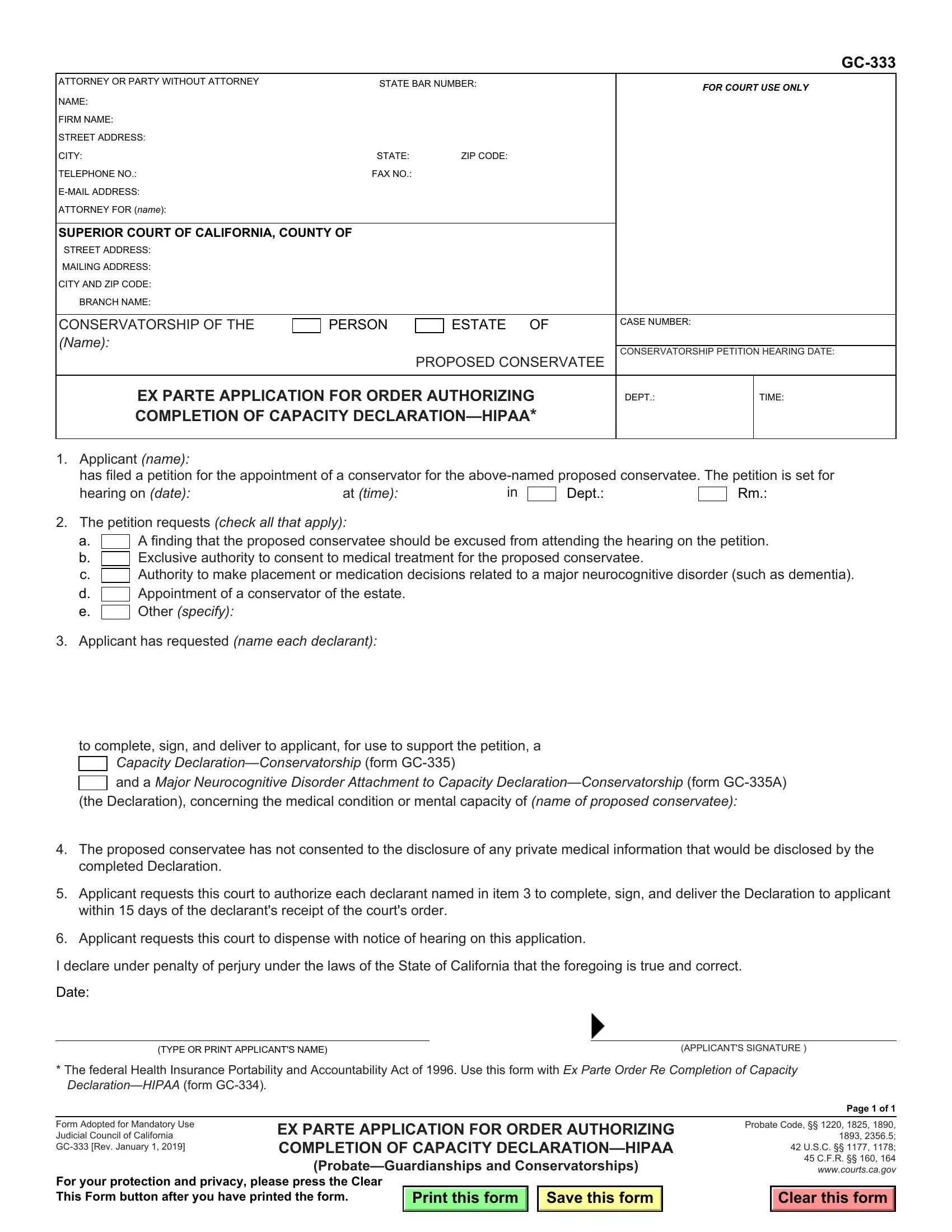
1. Before anything else, while filling out the california application order authorizing, begin with the part containing subsequent blanks:
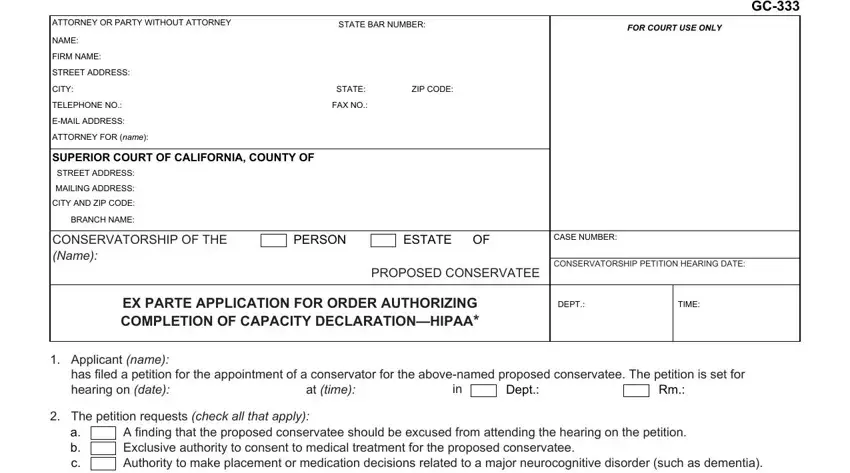
2. After filling out the previous part, go on to the subsequent part and enter the necessary particulars in all these blanks - a b c d e, A finding that the proposed, specify, Applicant has requested name each, to complete sign and deliver to, Capacity, the Declaration concerning the, The proposed conservatee has not, Applicant requests this court to, Applicant requests this court to, I declare under penalty of perjury, Date, TYPE OR PRINT APPLICANTS NAME, and APPLICANTS SIGNATURE.
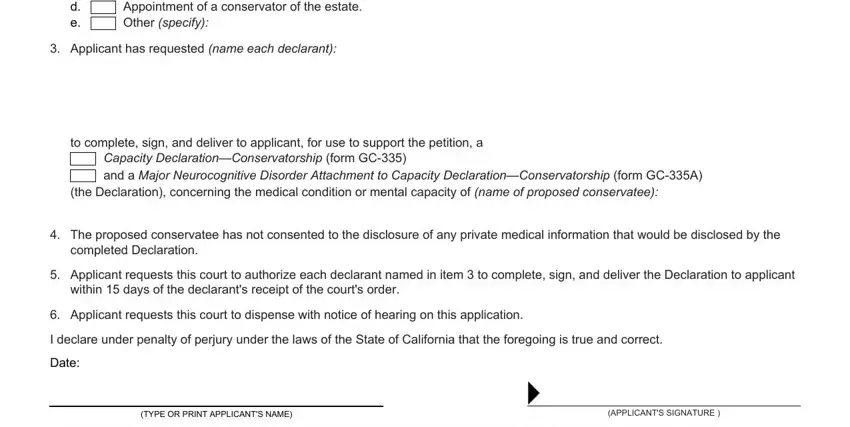
Always be extremely attentive when filling in A finding that the proposed and to complete sign and deliver to, as this is where most users make mistakes.
Step 3: As soon as you've reread the details provided, click "Done" to finalize your FormsPal process. Find your california application order authorizing once you register at FormsPal for a 7-day free trial. Easily access the pdf within your FormsPal account page, with any modifications and adjustments conveniently saved! FormsPal offers risk-free form editing without data record-keeping or distributing. Rest assured that your information is safe with us!