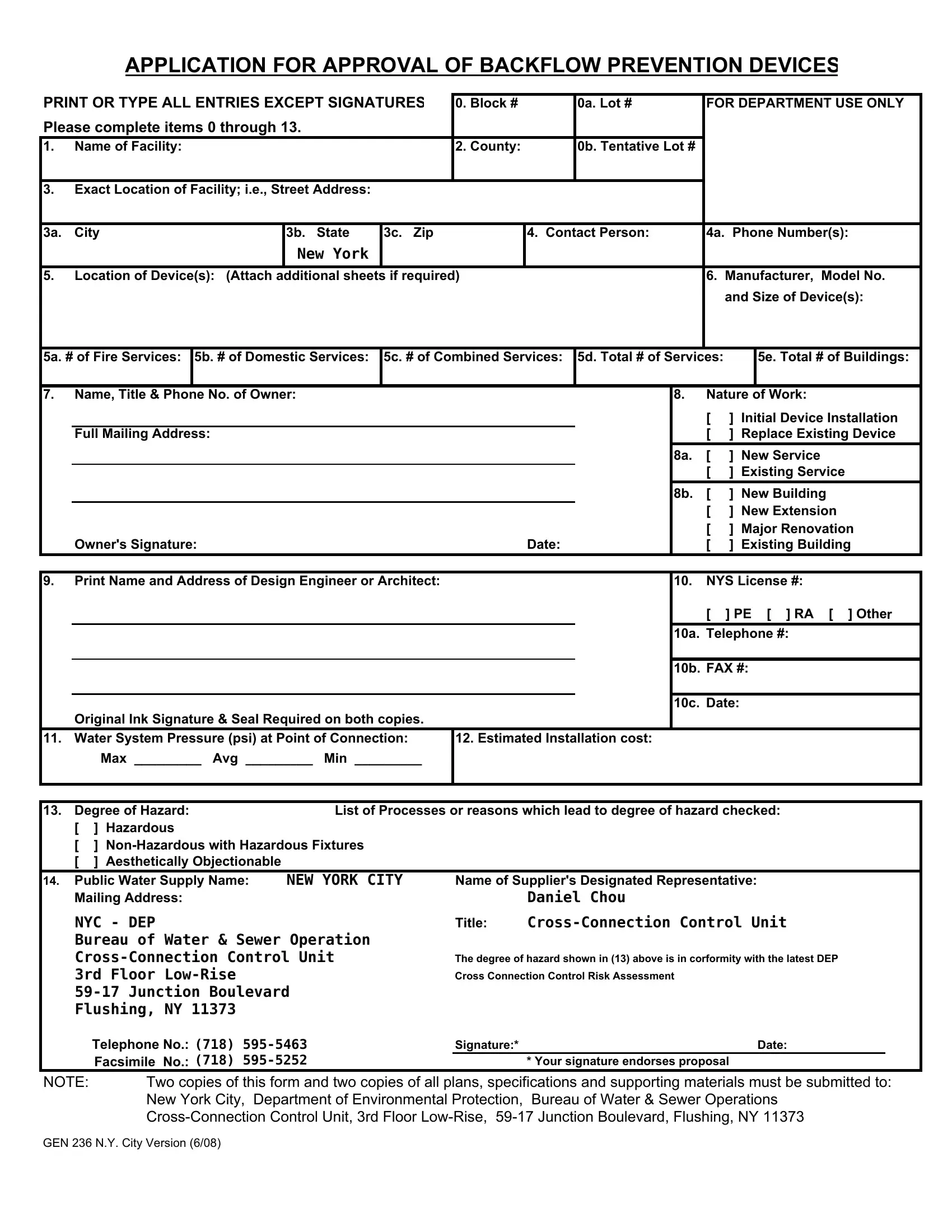
The Gen 236 form serves as a crucial document for any facility in New York City that needs to install, replace, or make any modifications to backflow prevention devices. This form, required by the New York City Department of Environmental Protection, is meticulously designed to gather comprehensive details about the facility, the specific backflow prevention devices being considered, and the justification for their installation based on the assessed degree of hazard. Facilities must provide information ranging from the exact location and contact details to specifics about the devices such as the manufacturer, model number, and size. Additionally, the form delves into the nature of the work being carried out – whether it's an initial installation, a replacement, or a new service – and requires insights into the system pressure, the estimated cost of installation, and the degree of hazard. This detailed documentation is essential for ensuring that water supplies remain uncontaminated by preventing backward flow which could potentially introduce hazardous materials. The task of filling out the Gen 236 form, thus, not only complies with regulatory measures but significantly contributes to public health and safety by maintaining the integrity of the water system.
| Question | Answer |
|---|---|
| Form Name | Form Gen 236 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 9 backflow prevention device nycdep form |
APPLICATION FOR APPROVAL OF BACKFLOW PREVENTION DEVICES
PRINT OR TYPE ALL ENTRIES EXCEPT SIGNATURES |
0. Block # |
|
0a. Lot # |
FOR DEPARTMENT USE ONLY |
||||||||||||
Please complete items 0 through 13. |
|
|
|
|
|
|
|
|
|
|
|
|||||
1. |
Name of Facility: |
|
|
|
2. County: |
|
0b. Tentative Lot # |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
3. |
Exact Location of Facility; i.e., Street Address: |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
3a. |
City |
|
3b. State |
3c. Zip |
|
4. Contact Person: |
4a. Phone Number(s): |
|||||||||
|
|
|
|
|
New York |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
5. |
Location of Device(s): (Attach additional sheets if required) |
|
|
|
6. |
Manufacturer, |
Model No. |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
and Size of Device(s): |
||||
|
|
|
|
|
|
|
|
|
|
|
||||||
5a. # of Fire Services: |
5b. # of Domestic Services: |
5c. # of Combined Services: |
5d. Total # of Services: |
|
|
5e. Total # of Buildings: |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
7. |
Name, Title & Phone No. of Owner: |
|
|
|
|
8. |
Nature of Work: |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
[ |
] |
Initial Device Installation |
|||
|
Full Mailing Address: |
|
|
|
|
|
|
|
[ |
] |
Replace Existing Device |
|||||
|
|
|
|
|
|
|
|
|
|
8a. |
[ |
] New Service |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
[ |
] |
Existing Service |
|||
|
|
|
|
|
|
|
|
|
|
8b. |
[ |
] New Building |
||||
|
|
|
|
|
|
|
|
|
|
|
[ |
] New Extension |
||||
|
|
|
|
|
|
|
|
|
|
|
[ |
] Major Renovation |
||||
|
Owner's Signature: |
|
|
|
|
Date: |
|
[ |
] |
Existing Building |
||||||
|
|
|
|
|
|
|
|
|
|
|||||||
9. |
Print Name and Address of Design Engineer or Architect: |
|
|
|
10. |
NYS License #: |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
[ |
] PE [ ] RA |
[ ] Other |
|||
|
|
|
|
|
|
|
|
|
|
10a. |
Telephone #: |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
10b. |
FAX #: |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10c. |
Date: |
|
|
|
|
|
|
Original Ink Signature & Seal Required on both copies. |
|
|
|
|
|
|
|
|
|
|
|||||
11. |
Water System Pressure (psi) at Point of Connection: |
12. Estimated Installation cost: |
|
|
|
|
|
|
||||||||
|
|
Max _________ Avg _________ Min _________ |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|||||||
13. |
Degree of Hazard: |
|
List of Processes or reasons which lead to degree of hazard checked: |
|
|
|||||||||||
|
[ |
] Hazardous |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
[ |
] |
|
|
|
|
|
|
|
|
|
|
|
|||
|
[ |
] Aesthetically Objectionable |
|
|
|
|
|
|
|
|
|
|
|
|||
14. |
Public Water Supply Name: |
|
NEW YORK CITY |
Name of Supplier's Designated Representative: |
|
|
||||||||||
|
Mailing Address: |
|
|
|
|
Daniel Chou |
|
|
|
|
|
|
||||
|
NYC - DEP |
|
|
|
Title: |
|
|
|||||||||
|
Bureau of Water & Sewer Operation |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
The degree of hazard shown in (13) above is in corformity with the latest DEP |
||||||||||||||
|
3rd Floor |
|
|
|
Cross Connection Control Risk Assessment |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Flushing, NY 11373 |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Telephone No.: (718) |
|
Signature:* |
|
|
|
|
|
|
Date: |
|
|
|||
|
|
Facsimile No.: (718) |
|
|
* Your signature endorses proposal |
|
|
|
|
|||||||
NOTE: |
Two copies of this form and two copies of all plans, specifications and supporting materials must be submitted to: |
|||||||||||||||
|
|
New York City, |
Department of Environmental Protection, |
Bureau of Water & Sewer Operations |
|
|
||||||||||
|
|
|
|
|||||||||||||
GEN 236 N.Y. City Version (6/08)
INSTRUCTION FOR FORM GEN 236 (NYC VERSION)
APPLICATION FOR APPROVAL OF BACKFLOW PREVENTION DEVICES
0 to 4a) Fill in as appropriate. Be sure to include the block and lot numbers.
5)Be as specific as possible, e.g. “8’ N of Elm Street and 12’ South of Main Street”
5a,b,c) |
Fill in the number of services for the entire facility. |
5d) |
This is the total of 5a,b, and c. |
5e) |
Fill in the total number of buildings in the facility. All adjacent buildings under |
|
the same ownership, occupancy or operation are considered part of the facility. |
|
Distant buildings with the same water, heating or other shared, common or |
|
interconnected systems are considered part of the same facility. If you have |
|
doubts or uncertainties, feel free to elaborate at length on additional sheets. |
6)Note Manufacturer, model & size of each device.
7)Indicate name, title & phone number of owner. Be sure to include the zip code and the original ink signature on both copies.
8,a,b) |
Check the appropriate spaces. |
9)Print name of the design engineer or architect. (Do not use the name of the firm in place of the P.E.’s or R.A.’s name). Fill in the complete address. Include the firm name if you wish.
Be sure to use original ink signatures and seals on both copies.
10)Include NYS License number in blank. Check appropriate category.
10a,b) |
Be sure to enter all applicable phone/fax numbers. |
10c) |
Enter date application is signed. |
11)Make sure that water system pressure at point of connection is included.
12)Be sure to include these estimates. No blanks permitted. Use fair market value if you are working for free.
13)Choose one of the Degree of Hazard and list the reasons. If you decided to choose Double Check Valve Assembly (DCVA), you are required to give the proper reasons.
14)To be completed by Water Supplier.
If you need additional space, use the back or attach additional sheets. If so, please indicate “Continued on back” or “See Additional Sheets” as appropriate.
Revised (6/08)