Estate planning is an important part of any individual or family's financial security. While there are many estate planning options available, one tool that is often overlooked is a form known as Form H Mr 1097. This form allows you to provide specific instructions to your heirs about the distribution of your assets after your death. Here we will discuss some of the key benefits of using Form H Mr 1097 in your estate plan. For more information on estate planning and Form H Mr 1097, please visit our website or contact us today. We would be happy to answer any questions you may have!
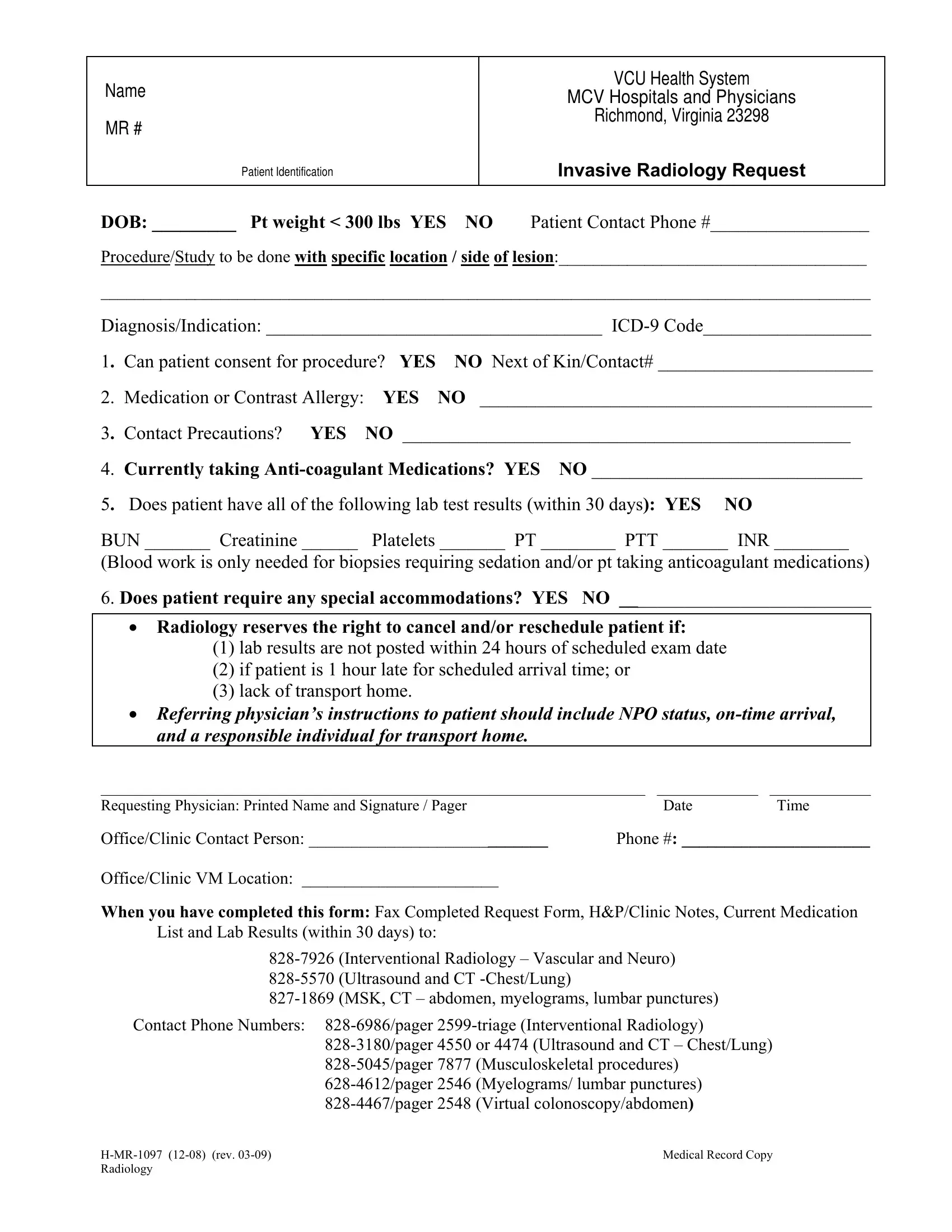
| Question | Answer |
|---|---|
| Form Name | Form H Mr 1097 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | InvasiveRadiolo gy mcv radiology email address form |
Name
MR #
Patient Identification
VCU Health System
MCV Hospitals and Physicians
Richmond, Virginia 23298
Invasive Radiology Request
DOB: _________ Pt weight < 300 lbs YES NO Patient Contact Phone #_________________
Procedure/Study to be done with specific location / side of lesion:____________________________________
__________________________________________________________________________________________
Diagnosis/Indication: ____________________________________
1. Can patient consent for procedure? YES |
NO Next of Kin/Contact# _______________________ |
||
2. |
Medication or Contrast Allergy: |
YES |
NO __________________________________________ |
3. Contact Precautions? YES |
NO ________________________________________________ |
||
4. |
Currently taking |
||
5. Does patient have all of the following lab test results (within 30 days): YES NO |
|||
BUN _______ Creatinine ______ |
Platelets _______ PT ________ PTT _______ INR ________ |
||
(Blood work is only needed for biopsies requiring sedation and/or pt taking anticoagulant medications)
6.Does patient require any special accommodations? YES NO ___________________________
•Radiology reserves the right to cancel and/or reschedule patient if:
(1)lab results are not posted within 24 hours of scheduled exam date
(2)if patient is 1 hour late for scheduled arrival time; or
(3)lack of transport home.
•Referring physician’s instructions to patient should include NPO status,
______________________________________________________________________ _____________ |
_____________ |
|
Requesting Physician: Printed Name and Signature / Pager |
Date |
Time |
Office/Clinic Contact Person: ____________________________ |
Phone #: ______________________ |
|
Office/Clinic VM Location: _______________________ |
|
|
When you have completed this form: Fax Completed Request Form, H&P/Clinic Notes, Current Medication List and Lab Results (within 30 days) to:
Contact Phone Numbers:
Medical Record Copy |
|
Radiology |
|