
benefits applying how download can be filled in in no time. Simply try FormsPal PDF editing tool to do the job right away. To keep our tool on the leading edge of efficiency, we strive to implement user-driven capabilities and enhancements on a regular basis. We are routinely looking for feedback - help us with revampimg the way you work with PDF documents. With just a couple of easy steps, you are able to begin your PDF journey:
Step 1: Click the "Get Form" button above on this webpage to open our PDF editor.
Step 2: This tool helps you customize almost all PDF files in a range of ways. Modify it by adding any text, adjust what's originally in the file, and include a signature - all doable in minutes!
In an effort to fill out this form, make certain you type in the information you need in every blank field:
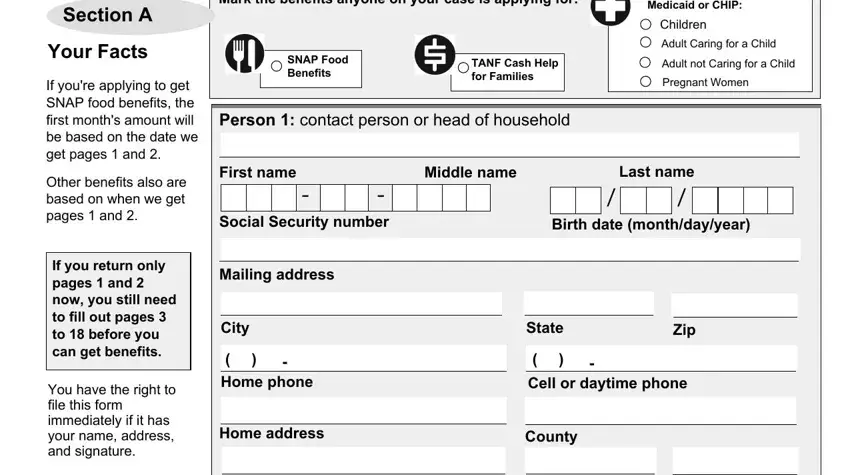
1. To start off, while completing the benefits applying how download, beging with the page that has the subsequent blank fields:
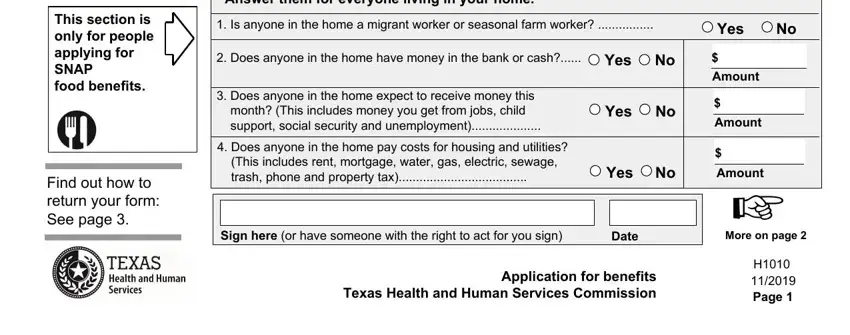
2. Right after completing the last step, go on to the next part and fill out the necessary details in all these blank fields - Food Benefits, This section is only for people, Find out how to return your form, You might be able to get SNAP food, Is anyone in the home a migrant, Yes, Does anyone in the home have, Yes, Does anyone in the home expect to, Does anyone in the home pay costs, Yes, Amount, Amount, Yes, and Amount.
Many people frequently make errors when filling in Amount in this part. Ensure that you read twice what you type in right here.
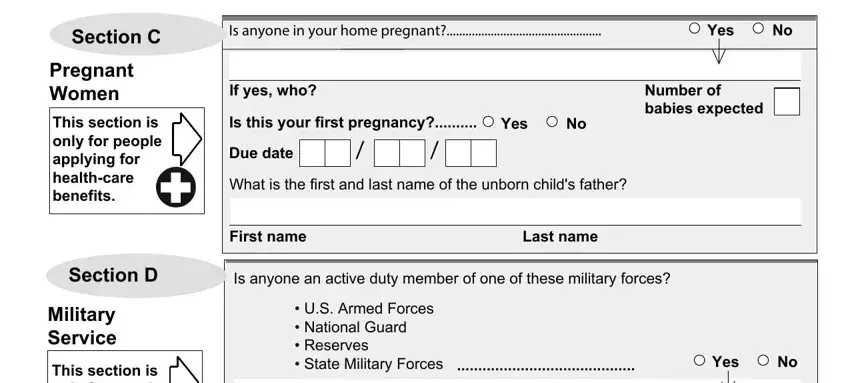
3. In this part, check out Section C, Pregnant Women, This section is only for people, Section D, Military Service, This section is only for people, Is anyone in your home pregnant, Yes, If yes who, Is this your first pregnancy, Yes, Due date, What is the first and last name of, Number of babies expected, and First name. Each of these have to be filled in with greatest focus on detail.
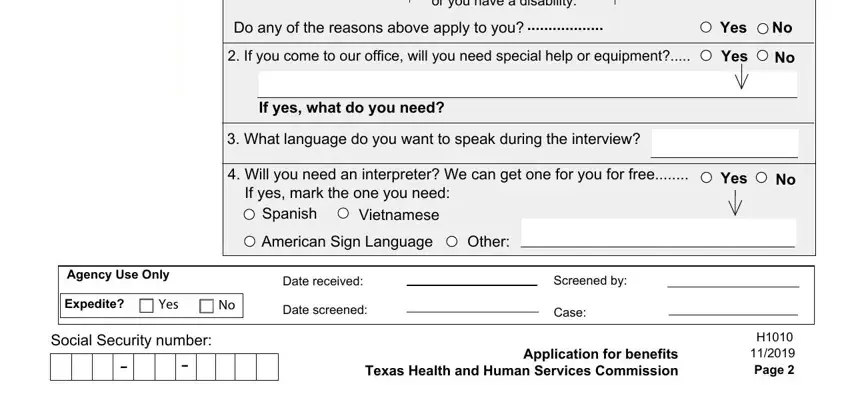
4. Filling in Your work or training hours dont, Do any of the reasons above apply, If you come to our office will, Yes, Yes, If yes what do you need, What language do you want to, Will you need an interpreter We, Yes, Spanish, Vietnamese, American Sign Language, Other, Agency Use Only, and Expedite is key in this fourth section - always take the time and take a close look at each and every field!
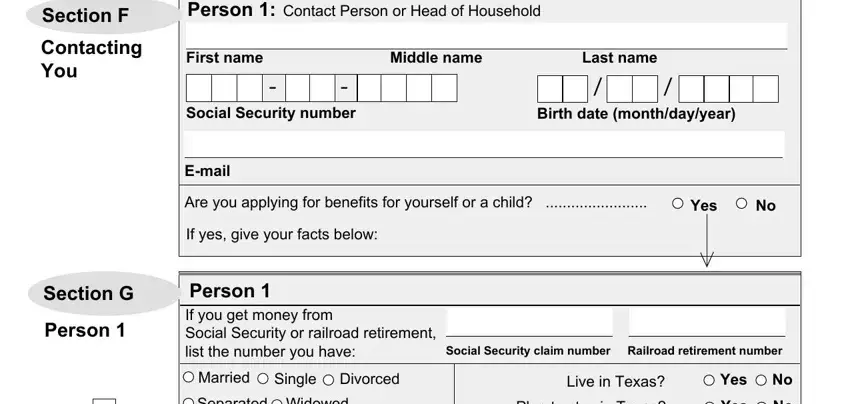
5. To finish your document, this last part incorporates a couple of additional fields. Filling in Section F, Contacting You, Person Contact Person or Head of, First name, Middle name, Social Security number, Last name, Birth date monthdayyear, Email, Are you applying for benefits for, Yes, Section G, Person, If yes give your facts below, and Person If you get money from will certainly finalize everything and you'll definitely be done in the blink of an eye!
Step 3: After you've looked again at the details in the blanks, click "Done" to complete your form. Make a free trial subscription with us and get immediate access to benefits applying how download - which you may then start using as you wish from your FormsPal cabinet. Here at FormsPal, we do everything we can to make certain that all of your details are kept private.