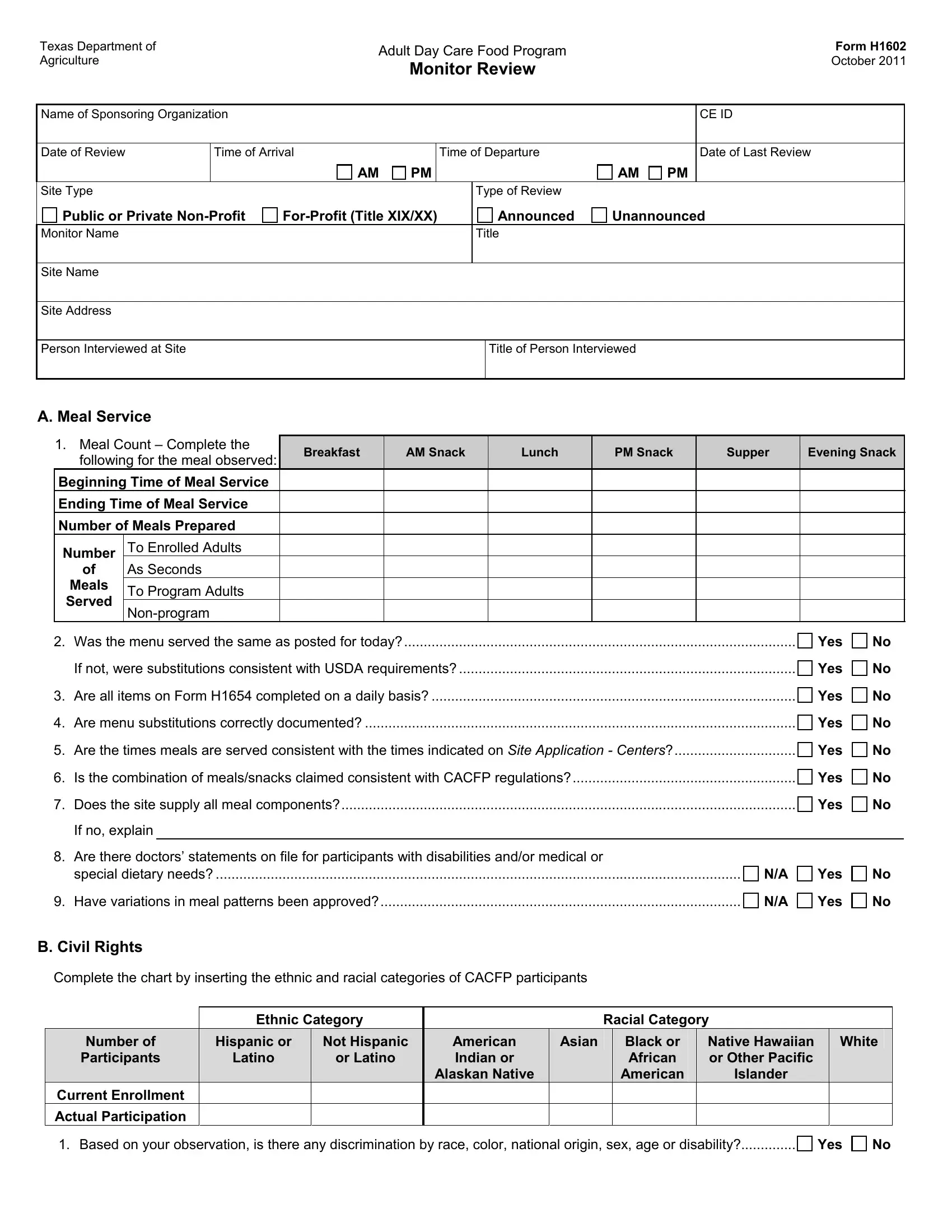
The H1602 form is a comprehensive document used by the Texas Department of Agriculture for monitoring Adult Day Care Food Programs. This form, updated in October 2011, serves as a critical tool in reviewing the operations of sponsoring organizations, ensuring compliance with both state and federal regulations. It captures detailed insights, ranging from meal service performance, civil rights adherence, and meal analysis to record-keeping standards, staff training, and five-day reconciliation of meal counts against attendance and enrollment. The form's structure facilitates a thorough assessment across various domains, including licensing certification display, correct meal counting procedures, participant enrollment verification, and eligibility for free or reduced-price meals. Notably, the H1602 form also investigates whether previous monitoring findings were adequately addressed, alongside verification of essential training for site staff involved in the program. Civil rights compliance, ensuring nondiscrimination in service, forms a critical part of the review, alongside a nuanced meal analysis that checks against the Child and Adult Care Food Program (CACFP) handbook for meal patterns and portion sizes. This detailed approach underscores an overarching goal: to maintain high standards in the provision of nutritious meals to enrolled adults, alongside ensuring organizational and operational integrity within Texas' Adult Day Care Food Program.
| Question | Answer |
|---|---|
| Form Name | Form H1602 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | tda form h1602 instructions, H1602, tda form 1602, XIX |
Texas Department of |
Adult Day Care Food Program |
|
|
|
Form H1602 |
||||||||||||||
Agriculture |
|
|
|
|
|
|
|
October 2011 |
|||||||||||
|
|
|
|
|
|
Monitor Review |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Name of Sponsoring Organization |
|
|
|
|
|
|
|
|
|
CE ID |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Review |
|
|
Time of Arrival |
|
Time of Departure |
|
|
Date of Last Review |
|
||||||||||
|
|
|
|
|
|
|
|
AM |
PM |
|
|
|
|
AM |
PM |
|
|
|
|
Site Type |
|
|
|
|
|
|
|
|
Type of Review |
|
|
|
|
|
|||||
|
Public or Private |
|
Announced |
Unannounced |
|
|
|||||||||||||
Monitor Name |
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Site Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Site Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Person Interviewed at Site |
|
|
|
|
|
Title of Person Interviewed |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
A. Meal Service |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
1. Meal Count – Complete the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Breakfast |
|
AM Snack |
|
Lunch |
|
PM Snack |
Supper |
Evening Snack |
|||||||||
|
|
following for the meal observed: |
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Beginning Time of Meal Service |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Ending Time of Meal Service |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Number of Meals Prepared |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Number |
|
To Enrolled Adults |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
of |
|
As Seconds |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Meals |
|
To Program Adults |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Served |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
2. |
Was the menu served the same as posted for today? |
.................................................................................................... |
|
|
|
|
|
|
|
Yes |
No |
||||||||
|
|
If not, were substitutions consistent with USDA requirements? |
|
|
|
|
|
|
Yes |
No |
|||||||||
3. |
Are all items on Form H1654 completed on a daily basis? |
|
|
|
|
|
|
Yes |
No |
||||||||||
4. |
Are menu substitutions correctly documented? |
|
|
|
|
|
|
|
Yes |
No |
|||||||||
5. |
Are the times meals are served consistent with the times indicated on Site Application - Centers? |
|
Yes |
No |
|||||||||||||||
6. |
Is the combination of meals/snacks claimed consistent with CACFP regulations? |
|
|
Yes |
No |
||||||||||||||
7. |
Does the site supply all meal components? |
|
|
|
|
|
|
|
Yes |
No |
|||||||||
|
|
If no, explain |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
8. |
Are there doctors’ statements on file for participants with disabilities and/or medical or |
|
|
|
|
|
|||||||||||||
|
|
special dietary needs? |
|
|
|
|
|
|
|
|
|
N/A |
Yes |
No |
|||||
9. |
Have variations in meal patterns been approved? |
|
|
|
|
|
|
N/A |
Yes |
No |
|||||||||
B. Civil Rights
Complete the chart by inserting the ethnic and racial categories of CACFP participants
|
Ethnic Category |
|
|
Racial Category |
|
|
|
|||
Number of |
Hispanic or |
Not Hispanic |
American |
Asian |
|
Black or |
Native Hawaiian |
|
White |
|
Participants |
Latino |
or Latino |
Indian or |
|
|
African |
or Other Pacific |
|
|
|
|
|
|
Alaskan Native |
|
|
American |
Islander |
|
|
|
Current Enrollment |
|
|
|
|
|
|
|
|
|
|
Actual Participation |
|
|
|
|
|
|
|
|
|
|
1. Based on your observation, is there any discrimination by race, color, national origin, sex, age or disability? |
Yes |
No |
||||||||
Form H1602
Page
C. Meal Analysis
1.Production: Complete the following information for the meal observed and calculate the amount of each component used. Consult the CACFP handbook for meal patterns.
|
Food Items Served |
Amount Prepared |
No. of Servings per |
Amount Needed |
+ OR - |
|
|
|
Amount Prepared |
|
|
Milk
Meat or Meat Alternative
Vegetables and/or Fruit (two or more)
Whole Grain or Enriched
Bread or Bread Alternative
Other Foods
2.Was a sufficient quantity of each component prepared to meet meal pattern
requirements for the number of participants? ...............................................................................................................
Yes
No
3. Type of meal service:
Family Style
Unit (Cafeteria Style)
Offer vs. Serve
4.Were all required components served? .......................................................................................................
5.Describe what happens to plate waste and leftovers.
Yes No
D. Record Keeping
1.Licensing
a.Is the current license/certification posted?
b.What is the current licensed capacity? .............................................................................................................................................................................................................................
Yes No
c. Does today’s attendance exceed the capacity? ......................................................................................................
If yes, explain.
Yes No
d. Is the site subject to licensing standards other than DADS? ...................................................................................
2. Enrollment – Does each participant have an enrollment form on file? ..........................................................................
3. Attendance – Is attendance recorded daily on Form H1535 (Daily Meal Count and Attendance Record)?..................
4. Meal Count
a. Is Form H1535 (Daily Meal Count and Attendance Record) completed at the time of
meal services on a daily basis?...............................................................................................................................
b. Is the monthly meal count being recorded on Form H4502? ...................................................................................
5. Eligibility
a. Is there a current (completed within the last 12 months) CACFP Meal Benefit Income Eligibility Form
(Adult Care Form) for each participant claimed in free and
b. b. Are the participants being claimed in the correct eligibility category (free,
including
c. Is there adequate documentation to ensure that at least 25% of the total enrollment or
licensed capacity received Title XIX/XX benefits?
d. If a pricing program, is there any indication of overt identification? .........................................................................
Yes No
Yes No
Yes No
Yes No Yes No
Yes No
Yes No
Yes No Yes No
6. Previous Monitoring Reviews |
|
a. Were problems identified at the last monitoring review? |
N/A |
b. If yes, were they corrected? |
|
c. If no, why not? |
|
Form H1602
Page
Yes No
Yes No
7. Records Retention – Is the site maintaining records per TDA requirements/regulations? ............................................
Yes No
E. Training
1. Have site staff that perform key activities received CACFP training for the current Program Year? |
Yes |
No |
a. If yes, is documentation on file that contains the required components? |
Yes |
No |
b. Were all required areas covered? |
Yes |
No |
c. If no, when is the site training scheduled?
2.If the site is new this Program Year, did the site staff that perform key activities receive
|
training over the required areas and subtopics before beginning the program? |
|
Yes |
No |
||
|
Is there documentation of file that contains the required components? |
|
Yes |
No |
||
F. |
|
|
|
|
||
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Compare Meal Counts to Attendance and Enrollment |
|
|
||
|
|
|
|
|
|
|
|
Date: |
Date: |
Date: |
Date: |
Date: |
|
|
B Meal Count = |
B Meal Count = |
B Meal Count = |
B Meal Count = |
B Meal Count = |
|
|
AM Meal Count = |
AM Meal Count = |
AM Meal Count = |
AM Meal Count = |
AM Meal Count = |
|
|
L Meal Count = |
L Meal Count = |
L Meal Count = |
L Meal Count = |
L Meal Count = |
|
|
PM Meal Count = |
PM Meal Count = |
PM Meal Count = |
PM Meal Count = |
PM Meal Count = |
|
|
S Meal Count = |
S Meal Count = |
S Meal Count = |
S Meal Count = |
S Meal Count = |
|
|
E Meal Count = |
E Meal Count = |
E Meal Count = |
E Meal Count = |
E Meal Count = |
|
|
Attendance = |
Attendance = |
Attendance = |
Attendance = |
Attendance = |
|
|
Enrollment = |
Enrollment = |
Enrollment = |
Enrollment = |
Enrollment = |
|
F.
2. Are there any days when meal counts by type exceed attendance? ............................................................................
a. If yes, what is the explanation?
Form H1602
Page
Yes No
b.Is the explanation reasonable?................................................................................................................................
i.If no, do meals need to be disallowed? ..............................................................................................................
ii.Document by type the number of meals disallowed.
Yes No
Yes No
3. Are there any days when meal counts by type exceed enrollment? .............................................................................
a. If yes, what is the explanation?
Yes No
b.Is the explanation reasonable?................................................................................................................................
i.If no, do meals need to be disallowed? ..............................................................................................................
ii.Document by type the number of meals disallowed.
Yes No
Yes No
G. Findings, Recommendations and Commendations
1.List problems identified. Document areas in which the site is performing well.
2.Recommendation – Indicate corrective action needed:
H. Signature
Signature – Monitor |
Date |
Signature – Site Representative |
Date |