
Whenever you need to fill out 1836b form, you don't have to download and install any software - simply try our PDF tool. In order to make our tool better and simpler to utilize, we continuously design new features, taking into consideration feedback coming from our users. To get the ball rolling, consider these easy steps:
Step 1: Access the PDF form inside our editor by clicking on the "Get Form Button" above on this webpage.
Step 2: The editor will allow you to modify your PDF in various ways. Improve it by adding personalized text, correct what's already in the PDF, and include a signature - all within the reach of a couple of mouse clicks!
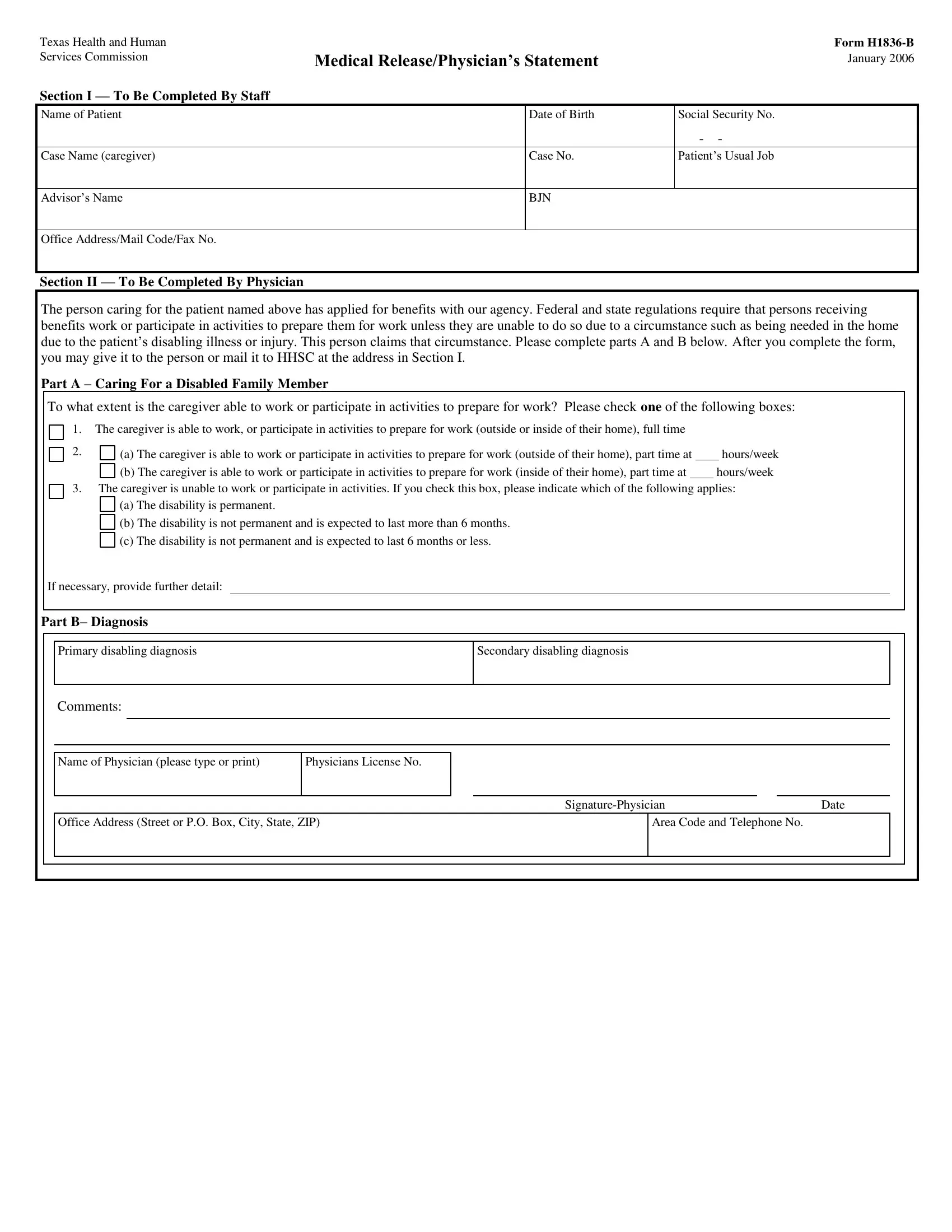
If you want to fill out this PDF form, make certain you provide the right details in each blank:
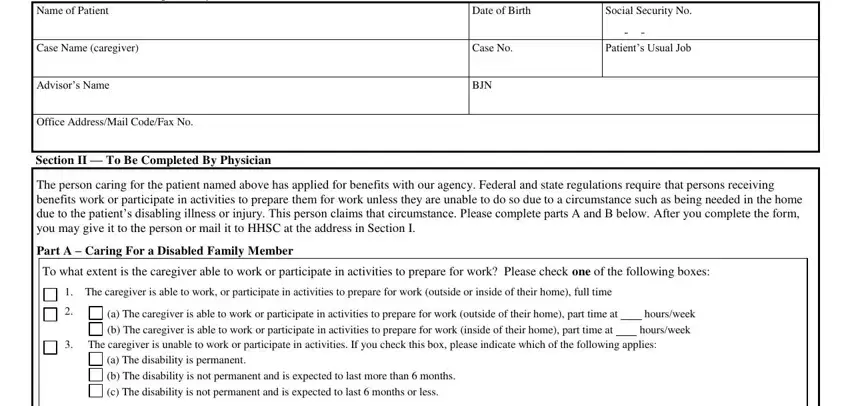
1. It is very important fill out the 1836b form properly, thus be careful when filling in the areas that contain all of these blanks:
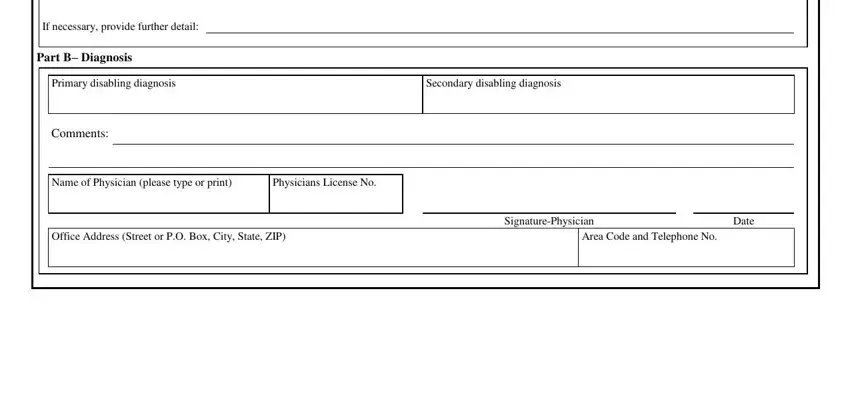
2. The third step is to fill in all of the following fields: If necessary provide further detail, Part B Diagnosis, Primary disabling diagnosis, Comments, Secondary disabling diagnosis, Name of Physician please type or, Physicians License No, Office Address Street or PO Box, SignaturePhysician, Date, and Area Code and Telephone No.
3. This next stage is going to be simple - fill in all the blanks in Section III To Be Completed By, Patients Name, The applicant is requesting an, I authorize, Doctor Medical Facilities or other, to complete Form HB Medical, This authorization expires on, Patient or Personal, Date, If you are signing for the patient, Note If the person requesting the, Witness, and Date to finish this process.
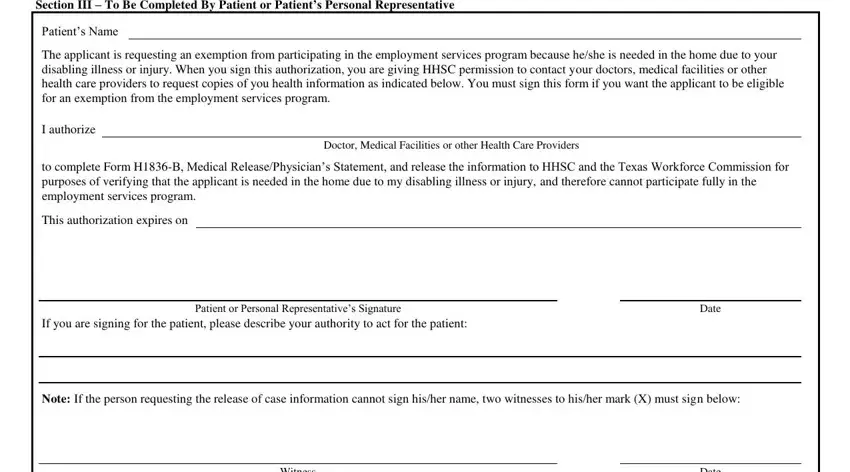
It is easy to make a mistake when filling in your Patient or Personal, thus make sure that you reread it before you'll send it in.
4. Completing Notice to Client, Witness, Date, HHSC as receiver of this, and You can withdraw permission you is key in the next step - make certain that you spend some time and take a close look at every blank area!
Step 3: Immediately after looking through the fields you've filled in, press "Done" and you're all set! Find the 1836b form after you register here for a free trial. Easily view the form within your FormsPal account, with any edits and adjustments being conveniently kept! We do not share or sell any details that you provide when dealing with forms at FormsPal.