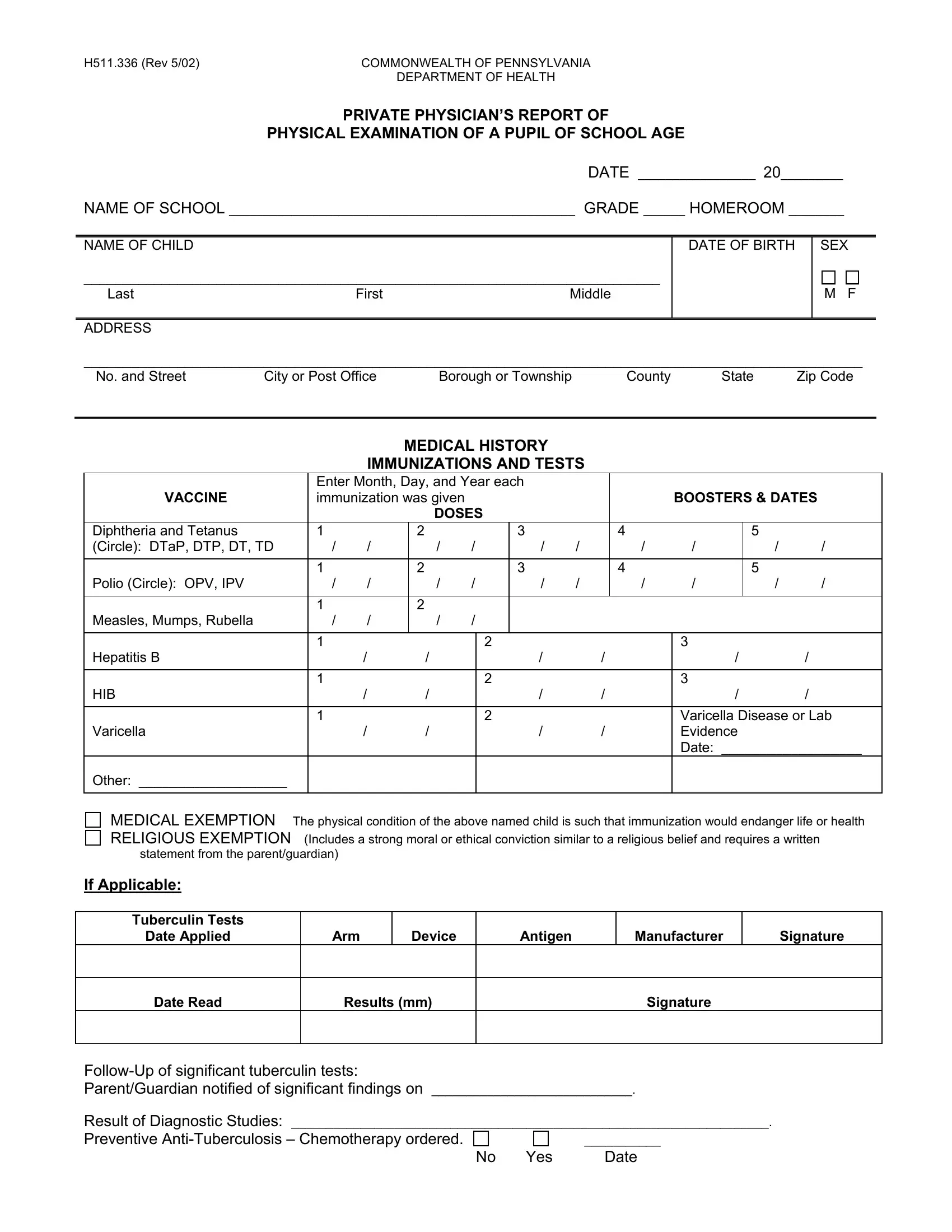
In the Commonwealth of Pennsylvania, ensuring that students of school age undergo a comprehensive physical examination is crucial for their well-being and educational success. The H511 336 form, devised by the Pennsylvania Department of Health, serves as the standardized document for private physicians to report these essential physical examinations. This form encompasses a wide variety of information starting with basic identification details of the student, including name, date of birth, and address. Importantly, it delves into the student's medical history, immunizations, and tests received by detailing the type and date of each vaccine administered, alongside booster shots. The form thoughtfully includes sections for medical and religious exemptions, particularly for cases where immunization might pose a risk to the child's health or conflict with familial beliefs. Furthermore, it requires details on significant medical conditions, covering a broad spectrum from allergies to neuromuscular disorders, aiming to highlight any special medical concerns that might necessitate restricted activity, medication, or could impact the student's education process. The form culminates with the physician's report of the physical examination, offering a concise overview of the pupil's health across various physiological parameters. Through this detailed reporting, the H511 336 form plays a pivotal role in safeguarding the health of Pennsylvania's school-aged children, ensuring they receive the proper care and considerations needed for a conducive learning environment.
| Question | Answer |
|---|---|
| Form Name | Form H511 336 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | DTaP, H511, pa school physical form h511 336, physical form for school pa |