In the landscape of employment within the educational sector of Pennsylvania, the health and safety of school personnel stand as pivotal factors ensuring a thriving environment for both staff and students. Among the plethora of forms and documents required, the H511 340 form emerges as a crucial piece in this vital framework. Officially recognized by the Commonwealth of Pennsylvania, this form, revised as of April 2000, serves as the standard school personnel health record, meticulously designed to compile comprehensive health data of employees within the educational domain. It encapsulates various segments including personal information, immunization history, tuberculosis test results, significant medical conditions, and a detailed report of physical examination. This form not only underscores the importance of maintaining a record of vaccinations such as Diphtheria, Tetanus, Hepatitis B, and MMR but also emphasizes the need for monitoring potential medical conditions that may influence an individual’s capability to fulfill their role effectively. The inclusion of a section dedicated to tuberculosis—highlighting the requirement for a test, subsequent results, and necessary follow-ups if a significant reaction is discovered—reflects the thoroughness with which the Pennsylvania Department of Health approaches public health within educational settings. Furthermore, the form thoughtfully provides space for the disclosure of any special medical problems or chronic diseases, ensuring that any condition which could necessitate restrictions or special considerations in the workplace is documented and communicated. As part of the employment process, this document acts not merely as a bureaucratic step but as a testament to the commitment to health and safety in Pennsylvania's educational institutions.
| Question | Answer |
|---|---|
| Form Name | Form H511 340 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | pa school personnel health record form, DTP, PENNSYLVANIA, Adventitous |
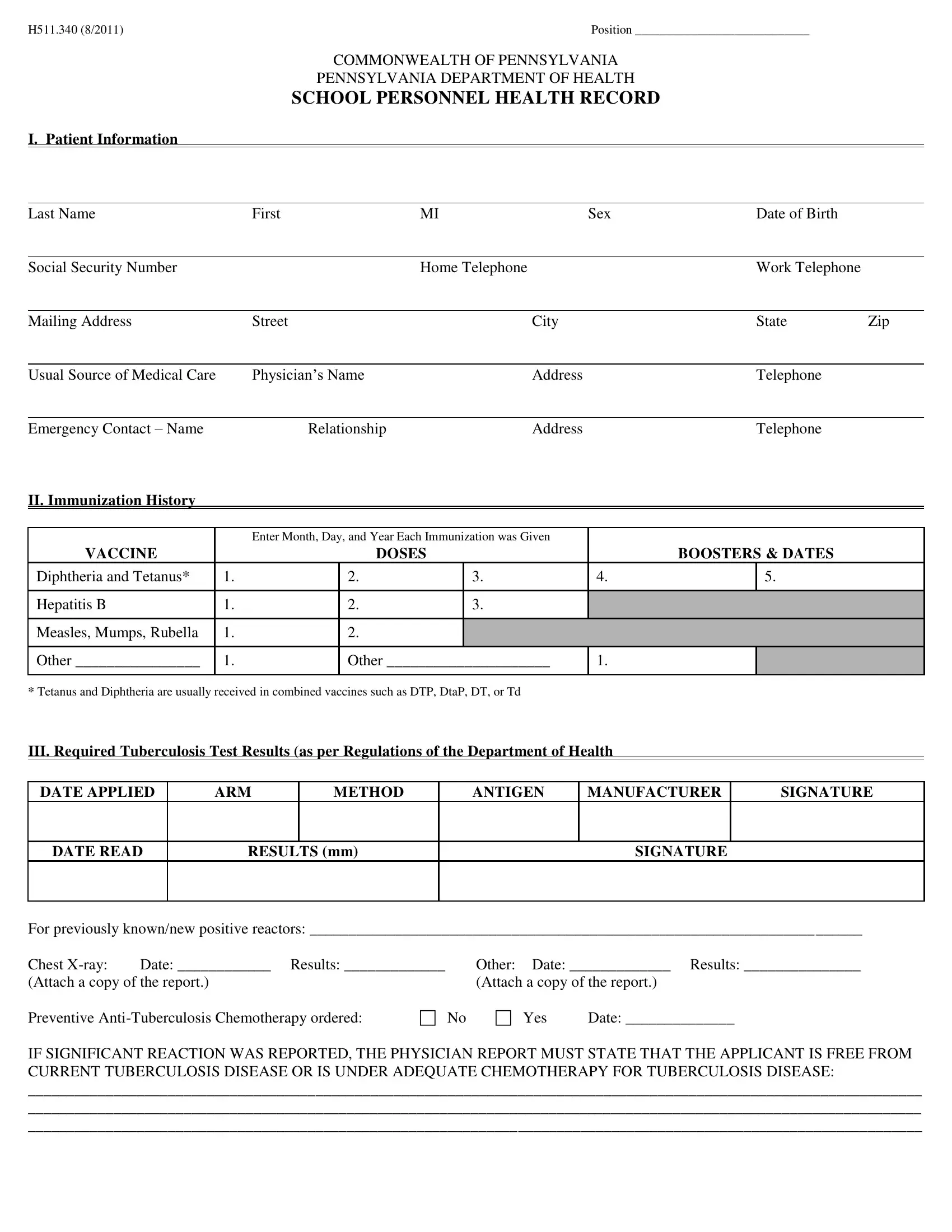
H511.340 (Rev. 4/00) |
Position ____________________________ |
COMMONWEALTH OF PENNSYLVANIA
PENNSYLVANIA DEPARTMENT OF HEALTH
SCHOOL PERSONNEL HEALTH RECORD
I. Patient Information
Last Name |
|
First |
MI |
Sex |
|
Date of Birth |
|
|||
|
|
|
|
|
|
|
|
|
|
|
Social Security Number |
|
|
|
Home Telephone |
|
|
Work Telephone |
|
||
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
Street |
|
City |
|
|
State |
Zip |
||
|
|
|
|
|
|
|
|
|
|
|
Usual Source of Medical Care |
|
Physician’s Name |
|
Address |
|
|
Telephone |
|
||
|
|
|
|
|
|
|
|
|
|
|
Emergency Contact – Name |
|
Relationship |
|
Address |
|
|
Telephone |
|
||
II. Immunization History |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enter Month, Day, and Year Each Immunization was Given |
|
|
|
|
|||
VACCINE |
|
|
|
DOSES |
|
BOOSTERS & DATES |
|
|||
Diphtheria and Tetanus* |
|
1. |
|
2. |
|
3. |
4. |
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
Hepatitis B |
|
1. |
|
2. |
|
3. |
|
|
|
|
Measles, Mumps, Rubella |
|
1. |
|
2. |
|
|
|
|
|
|
Other ________________ |
|
1. |
|
Other _____________________ |
1. |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
*Tetanus and Diphtheria are usually received in combined vaccines such as DTP, DtaP, DT, or Td
III. Required Tuberculosis Test Results (as per Regulations of the Department of Health
DATE APPLIED |
ARM |
METHOD |
ANTIGEN |
MANUFACTURER |
SIGNATURE |
|
|
|
|
|
|
DATE READ
RESULTS (mm)
SIGNATURE
For previously known/new positive reactors: _______________________________________________________________________
Chest |
Date: ____________ Results: _____________ |
Other: |
Date: _____________ Results: _______________ |
|
(Attach a copy of the report.) |
(Attach a copy of the report.) |
|||
Preventive |
No |
Yes |
Date: ______________ |
|
IF SIGNIFICANT REACTION WAS REPORTED, THE PHYSICIAN REPORT MUST STATE THAT THE APPLICANT IS FREE FROM CURRENT TUBERCULOSIS DISEASE OR IS UNDER ADEQUATE CHEMOTHERAPY FOR TUBERCULOSIS DISEASE:
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
IV. Significant Medical Conditions ( ) |
|
|
|
|
|
Yes |
No |
If Yes, Explain: |
Allergies |
|
___________________________________________________________________ |
Asthma |
|
___________________________________________________________________ |
Cardiac |
|
___________________________________________________________________ |
Chemical Dependency |
|
___________________________________________________________________ |
Drugs |
|
___________________________________________________________________ |
Alcohol |
|
___________________________________________________________________ |
Diabetes Mellitus |
|
___________________________________________________________________ |
Gastrointestinal Disorder |
|
___________________________________________________________________ |
Hearing Disorder |
|
___________________________________________________________________ |
Hypertension |
|
___________________________________________________________________ |
Neuromuscular Disorder |
|
___________________________________________________________________ |
Orthopedic Condition |
|
___________________________________________________________________ |
Respiratory Illness |
|
___________________________________________________________________ |
Seizure Disorder |
|
___________________________________________________________________ |
Skin Disorder |
|
___________________________________________________________________ |
Vision Disorder |
|
___________________________________________________________________ |
Other (Specify) |
|
___________________________________________________________________ |
V. Report of Physical Examination ( )
|
NORMAL |
ABNORMAL |
NOT |
COMMENTS |
|
EXAMINED |
|||
|
|
|
|
|
Height (inches) ______________ |
|
|
|
|
|
|
|
|
|
Weight (pounds) ______________ |
|
|
|
|
Pulse _____________ |
|
|
|
|
|
|
|
|
|
Blood Pressure ______________ |
|
|
|
|
|
|
|
|
|
Hair/Scalp |
|
|
|
|
|
|
|
|
|
Skin |
|
|
|
|
Eyes – Visual Acuity: R _____ L _____ |
|
|
|
|
|
|
|
|
|
Eyes – Color Vision |
|
|
|
|
|
|
|
|
|
Ears – Hearing (dB) R _____ L _____ |
|
|
|
|
Nose and Throat |
|
|
|
|
|
|
|
|
|
Teeth and Gingiva |
|
|
|
|
|
|
|
|
|
Lymph Glands |
|
|
|
|
|
|
|
|
|
Heart – Murmur, etc… |
|
|
|
|
|
|
|
|
|
Lungs – Adventitous Findings |
|
|
|
|
|
|
|
|
|
Abdomen |
|
|
|
|
|
|
|
|
|
Genitourinary |
|
|
|
|
|
|
|
|
|
Neuromuscular System |
|
|
|
|
|
|
|
|
|
Extremities |
|
|
|
|
|
|
|
|
|
Are there any special medical problems or chronic diseases which require restriction of activity, medication or which might affect his/her work role? If so, specify __________________________________________________________________________________
____________________________________________ |
__________________________________________________ |
___________________ |
Physician Name (Print) |
Signature of Examiner |
Date |
______________________________________________________________________________________________________________________________
Physician Address
The statements and answers as recorded above are full, complete and true to the best of my knowledge and belief. I understand that any false or misleading statements may cause termination of my employment.
I authorize the physician or other person to disclose any knowledge or information pertaining to my health to the employing authority for whom this examination is performed.
_________________________________________ |
_____________________ |
Signature of Employee |
Date |