Navigating the complexities of health care needs and the requisite forms can be a daunting process for individuals requiring special medical supplies. Among these necessary forms is the HCA 13 870 form, a critical document designed primarily for individuals in need of incontinent supplies and gloves beyond the standard limitation. Specifically tailored towards those under durable medical equipment (DME) management, this form serves as a limitation extension request to ensure that individuals have adequate supplies for their medical condition. The process requires detailed information about the client, including medical diagnoses, frequency of product use, any recent changes in that frequency, and the involvement of medications or bowel/bladder programs that might influence the quantity of supplies needed. Additionally, it inquires about the client's living situation, the presence of non-family caregivers, and necessitates a completed HCA Rx form alongside. This document not only bridges the communication between vendors or clinicians and the DME Program Management Unit but also emphasizes confidentiality and the importance of regular updates to maintain the supply extension. By comprehensively assessing an individual's needs through the details requested in the form, it stands as a pivotal step in securing essential medical supplies for those whose conditions demand more than the standard provision.
| Question | Answer |
|---|---|
| Form Name | Form Hca 13 870 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 13_870 informationsharingconsent |
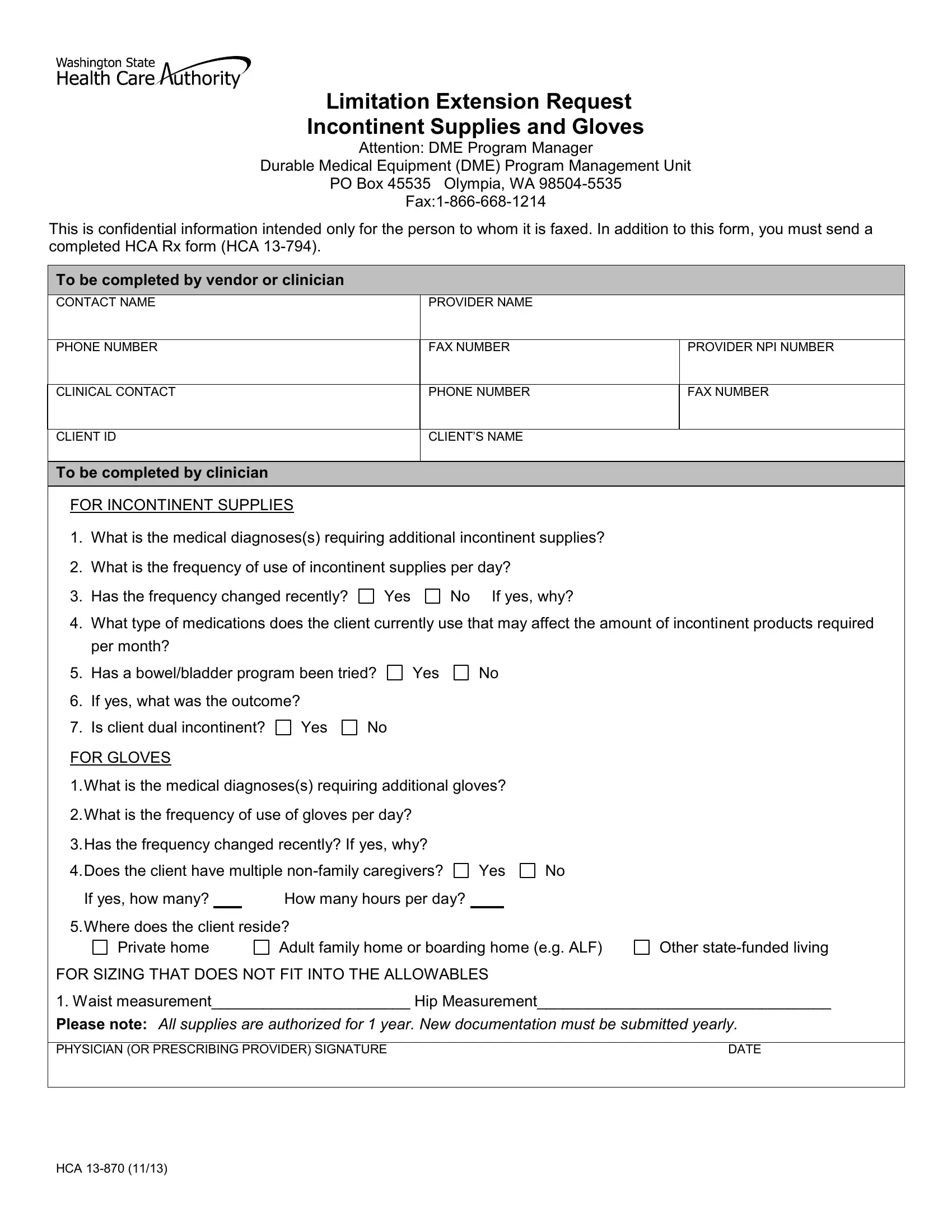
Limitation Extension Request
Incontinent Supplies and Gloves
Attention: DME Program Manager
Durable Medical Equipment (DME) Program Management Unit
PO Box 45535 Olympia, WA
This is confidential information intended only for the person to whom it is faxed. In addition to this form, you must send a completed HCA Rx form (HCA
To be completed by vendor or clinician
CONTACT NAME
PROVIDER NAME
PHONE NUMBER
FAX NUMBER
PROVIDER NPI NUMBER
CLINICAL CONTACT
PHONE NUMBER
FAX NUMBER
CLIENT ID
CLIENT’S NAME
To be completed by clinician
FOR INCONTINENT SUPPLIES
1.What is the medical diagnoses(s) requiring additional incontinent supplies?
2.What is the frequency of use of incontinent supplies per day?
3. Has the frequency changed recently?
Yes
No If yes, why?
4.What type of medications does the client currently use that may affect the amount of incontinent products required per month?
5.Has a bowel/bladder program been tried?
6.If yes, what was the outcome?
7.Is client dual incontinent? Yes No
FOR GLOVES
Yes
No
1.What is the medical diagnoses(s) requiring additional gloves?
2.What is the frequency of use of gloves per day?
3.Has the frequency changed recently? If yes, why?
4.Does the client have multiple
If yes, how many? |
|
How many hours per day? |
No
5.Where does the client reside?
Private home |
Adult family home or boarding home (e.g. ALF) |
FOR SIZING THAT DOES NOT FIT INTO THE ALLOWABLES
Other
1. Waist measurement_______________________ Hip Measurement__________________________________
Please note: All supplies are authorized for 1 year. New documentation must be submitted yearly.
PHYSICIAN (OR PRESCRIBING PROVIDER) SIGNATURE |
DATE |
|
|
HCA