Form Hcm 4 B is an important form for businesses in Vietnam. This form is used to declare employee benefits, and it must be filed with the Department of Social Welfare and Labor every month. Here's what you need to know about Form Hcm 4 B. This form is used to declare employee benefits, including allowances, bonuses, and other payments. The form must be filed with the Department of Social Welfare and Labor every month. Businesses in Vietnam are required to file this form, regardless of their size or type. There are a few things to keep in mind when filing Form Hcm 4 B. First, make sure that all information is accurate and up-to-date. Second, keep copies of the form for your records. Finally, make sure that the forms are submitted on time each month. Filing late can result in fines or other penalties. If you have any questions about Form Hcm 4 B or need help filing it correctly, contact the Department of Social Welfare and Labor for assistance. They will be happy to help you ge
| Question | Answer |
|---|---|
| Form Name | Form Hcm 4 B |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | opm 4b form |
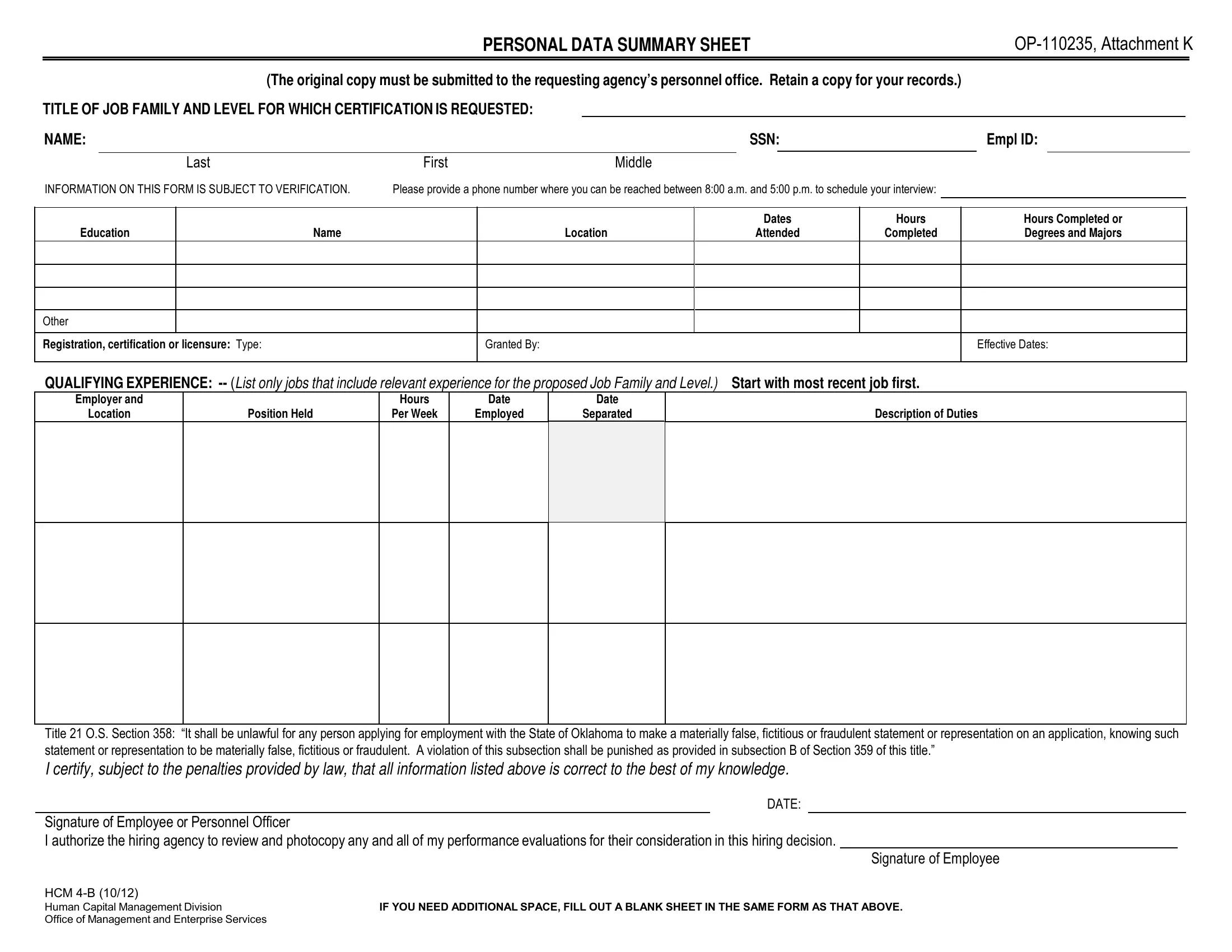
PERSONAL DATA SUMMARY SHEET |
||
|
|
|
(The original copy must be submitted to the requesting agency’s personnel office. Retain a copy for your records.)
TITLE OF JOB FAMILY AND LEVEL FOR WHICH CERTIFICATION IS REQUESTED:
NAME: |
|
|
SSN: |
Empl ID: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
Last |
First |
Middle |
|
|
|
|
|
|
INFORMATION ON THIS FORM IS SUBJECT TO VERIFICATION. |
Please provide a phone number where you can be reached between 8:00 a.m. and 5:00 p.m. to schedule your interview: |
|
|
|
|
||||
Education
Name
Location
Dates
Attended
Hours
Completed
Hours Completed or Degrees and Majors
Other |
|
Registration, certification or licensure: Type: |
Granted By: |
Effective Dates:
QUALIFYING EXPERIENCE:
Employer and
Location
Position Held
Hours
Per Week
Date
Employed
Date
Separated
Description of Duties
Title 21 O.S. Section 358: “It shall be unlawful for any person applying for employment with the State of Oklahoma to make a materially false, fictitious or fraudulent statement or representation on an application, knowing such statement or representation to be materially false, fictitious or fraudulent. A violation of this subsection shall be punished as provided in subsection B of Section 359 of this title.”
I certify, subject to the penalties provided by law, that all information listed above is correct to the best of my knowledge.
DATE:
Signature of Employee or Personnel Officer
I authorize the hiring agency to review and photocopy any and all of my performance evaluations for their consideration in this hiring decision.
Signature of Employee
HCM
Human Capital Management Division |
IF YOU NEED ADDITIONAL SPACE, FILL OUT A BLANK SHEET IN THE SAME FORM AS THAT ABOVE. |
Office of Management and Enterprise Services |
|
DEPARTMENT OF CORRECTIONS SUPPLEMENTAL PERSONAL DATA SUMMARY SHEET
NAME: |
|
|
SSN |
|
|
|
|
|
|
|
Last |
First |
Middle |
|
The Prison Rape Elimination Act (§115.17) requires that the Department of Corrections ask the following questions prior to hiring or promoting staff (please check a response to each question):
Have you ever engaged in sexual abuse in a prison, jail, lockup, community confinement facility, juvenile facility, or other institution? |
Yes |
Have you ever been convicted (or civilly or administratively adjudicated) of engaging or attempting to engage in sexual activity in |
Yes |
the community facilitated by force, overt or implied threats of force, or coercion, or if the victim did not consent or was unable to |
|
consent or refuse? |
|
Have you ever engaged in any incidents of sexual harassment? |
Yes |
If you answered yes to any question, please explain: _____________________________________________________________________ |
|
_______________________________________________________________________________________________________________ |
|
_______________________________________________________________________________________________________________ |
|
_______________________________________________________________________________________________________________ |
|
_______________________________________________________________________________________________________________ |
|
_______________________________________________________________________________________________________________ |
|
_______________________________________________________________________________________________________________ |
|
_______________________________________________________________________________________________________________ |
|
P.R.E.A. §115.17(g): “Material omissions regarding such misconduct, or the provision of materially false information, shall be grounds for termination.”
I certify, subject to the penalties provided by law, that all information listed above is correct to the best of my knowledge.
DATE:
Signature of Employee
No
No
No
DOC
IF YOU NEED ADDITIONAL SPACE, FILL OUT A BLANK SHEET IN THE SAME FORM AS THAT ABOVE.