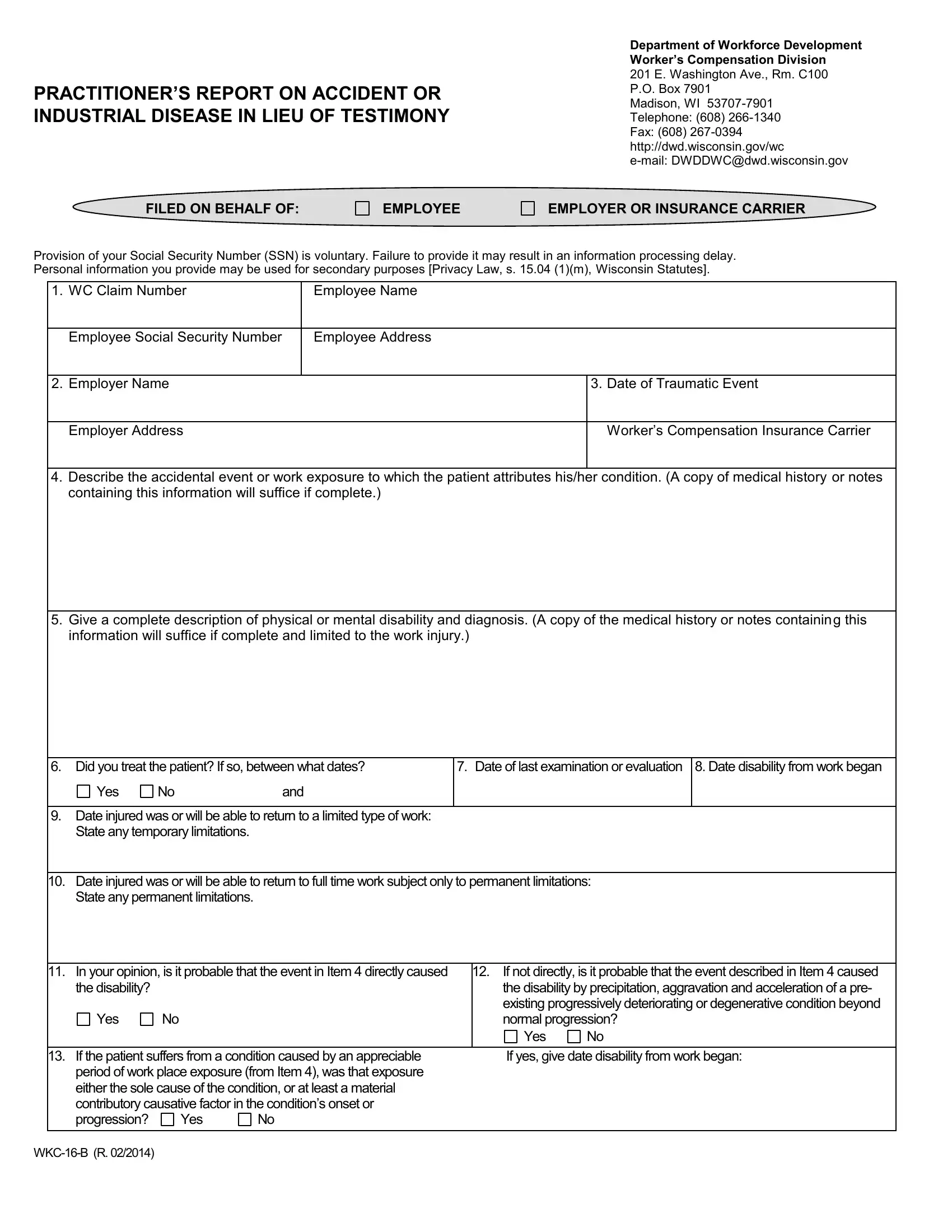
When workers in Wisconsin experience an accident or develop an industrial disease related to their workplace, navigating the aftermath can be challenging—both for them and the involved entities, such as employers and insurance carriers. The WKC 16 B form, also known as the Practitioner’s Report on Accident or Industrial Disease in Lieu of Testimony, serves as a crucial document within this context. Managed by the Department of Workforce Development Worker’s Compensation Division, this form allows medical practitioners to provide a detailed report covering the employee's condition, the treatment provided, and the prognosis. It requires detailed information about the employee, the employer, the specifics of the incidents, and the nature of the disabilities resulted from said incidents—whether they be physical or mental. The form also delves into questions about any permanent disabilities, the expected capacity for the employee to return to work, and the necessity of further treatment. This form is essential because it can be used as prima facie evidence in worker's compensation claims, streamlining the process and possibly eliminating the need for the doctor to provide oral testimony. The statutes set forth by Wisconsin law underscore the importance of this document in the claims process, making it a pivotal piece of documentation for all parties involved in worker’s compensation cases.
| Question | Answer |
|---|---|
| Form Name | Wkc 16 B Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form wkc 16 b, wkc 16 form, wisconsin workers compensation forms, wkc 16b pdf |
