

You may fill out SLF instantly with the help of our PDF editor online. To make our editor better and easier to utilize, we continuously come up with new features, considering feedback coming from our users. To start your journey, take these easy steps:
Step 1: Click the orange "Get Form" button above. It is going to open our editor so that you can begin filling out your form.
Step 2: This tool will allow you to modify almost all PDF files in a variety of ways. Modify it by including customized text, adjust existing content, and put in a signature - all when you need it!
When it comes to blanks of this precise form, here is what you want to do:
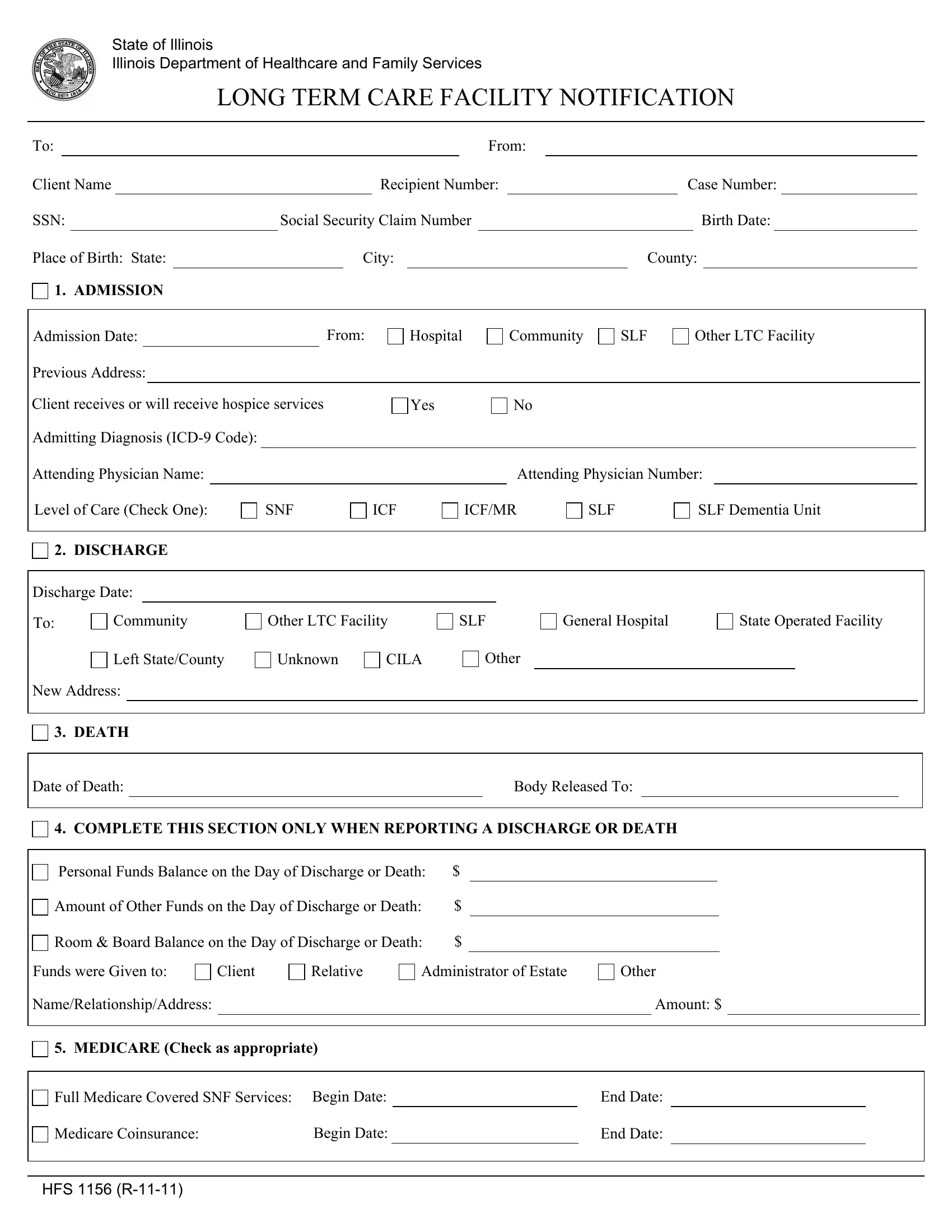
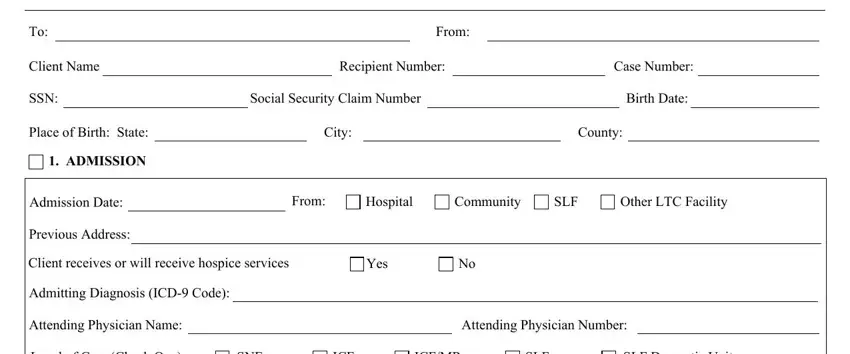
1. Begin filling out the SLF with a number of necessary blank fields. Get all of the important information and make sure not a single thing omitted!
2. Once your current task is complete, take the next step – fill out all of these fields - DISCHARGE, Discharge Date, Community, Other LTC Facility, SLF, General Hospital, State Operated Facility, Left StateCounty, Unknown, CILA, Other, New Address, DEATH, Date of Death, and Body Released To with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
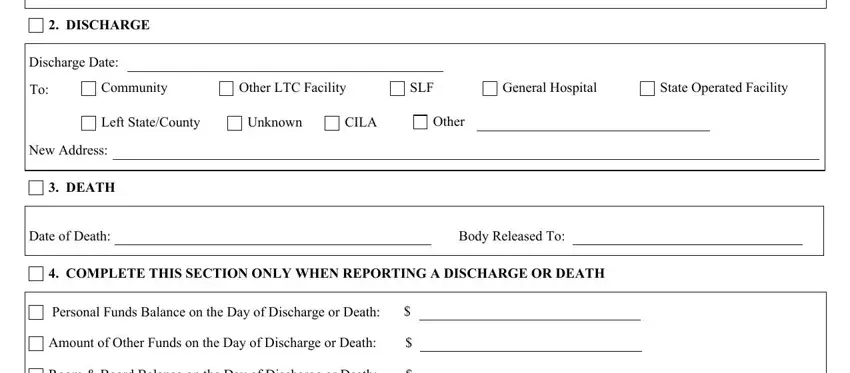
3. The following segment is about Room Board Balance on the Day of, Funds were Given to, Client, Relative, Administrator of Estate, Other, NameRelationshipAddress, Amount, MEDICARE Check as appropriate, Full Medicare Covered SNF Services, Medicare Coinsurance, Begin Date, End Date, End Date, and HFS R - type in all of these empty form fields.
Many people frequently make errors when completing End Date in this area. Make sure you read twice everything you enter here.
4. You're ready to proceed to this fourth section! Here you will get all of these INSURANCE COVERAGE TPL, eg name of company change in, RECEIPT OF LONG TERM CARE, Date Received, Amount, Dates Covered by Payment, Date and Amount of TPL Funds if, Date, Amount, Date and Amount of Group Care, Date, Amount, INCOME Check as appropriate, Change in Income, and Previous Monthly Amount form blanks to do.
5. To wrap up your form, the particular area includes several extra blank fields. Typing in HFS Attached, Yes, HFS Attached, Yes, SignatureTitle, Date, INSTRUCTIONS FOR COMPLETION, PURPOSE The HFS is used by the, because the clients funds have not, Check if reporting a change to or, and enter necessary information, This section is completed to, and Complete as needed should wrap up everything and you're going to be done in a flash!
Step 3: Before finishing this file, it's a good idea to ensure that blanks have been filled in the correct way. Once you’re satisfied with it, click “Done." Get hold of your SLF after you sign up for a free trial. Conveniently use the pdf document from your personal account, with any modifications and adjustments automatically saved! Here at FormsPal.com, we endeavor to make certain that all your information is kept protected.