
Dealing with PDF files online is definitely easy with this PDF tool. You can fill in hfs 2249 form here in a matter of minutes. The tool is consistently updated by us, receiving new awesome features and turning out to be better. With some basic steps, you can start your PDF journey:
Step 1: Simply click the "Get Form Button" at the top of this page to access our pdf editor. Here you'll find all that is needed to work with your file.
Step 2: Once you open the online editor, you will see the form all set to be filled in. Other than filling in various blanks, you might also do several other things with the Document, including adding your own text, editing the original textual content, inserting illustrations or photos, putting your signature on the PDF, and much more.
This form will need specific details; in order to guarantee consistency, please take note of the suggestions further down:
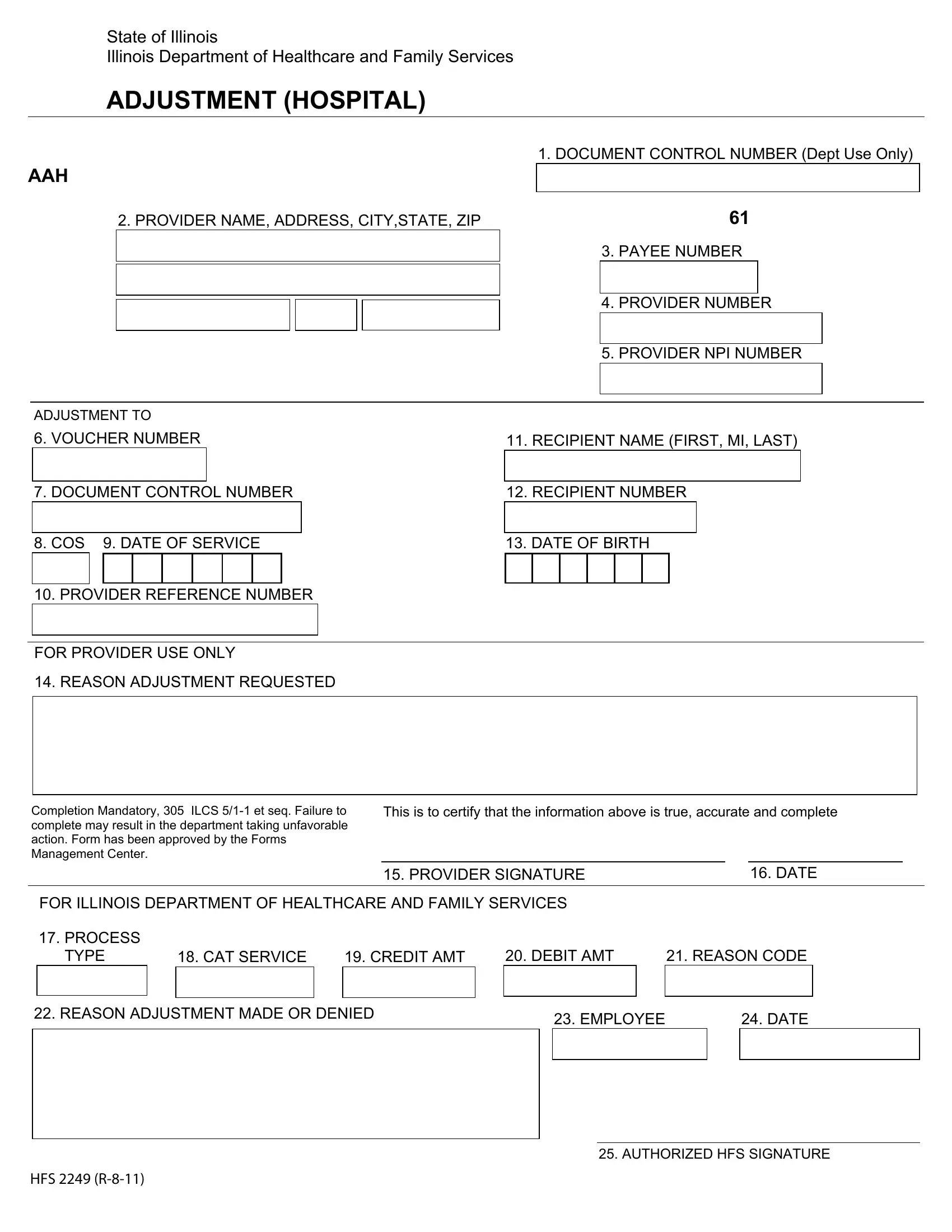
1. Begin completing the hfs 2249 form with a group of necessary blanks. Gather all of the required information and make certain not a single thing omitted!
2. After filling in this section, go on to the subsequent step and fill in the essential particulars in these fields - REASON ADJUSTMENT REQUESTED, Completion Mandatory ILCS et seq, This is to certify that the, FOR ILLINOIS DEPARTMENT OF, PROCESS TYPE, CAT SERVICE, CREDIT AMT, DEBIT AMT, REASON CODE, PROVIDER SIGNATURE, DATE, REASON ADJUSTMENT MADE OR DENIED, EMPLOYEE, DATE, and HFS R.
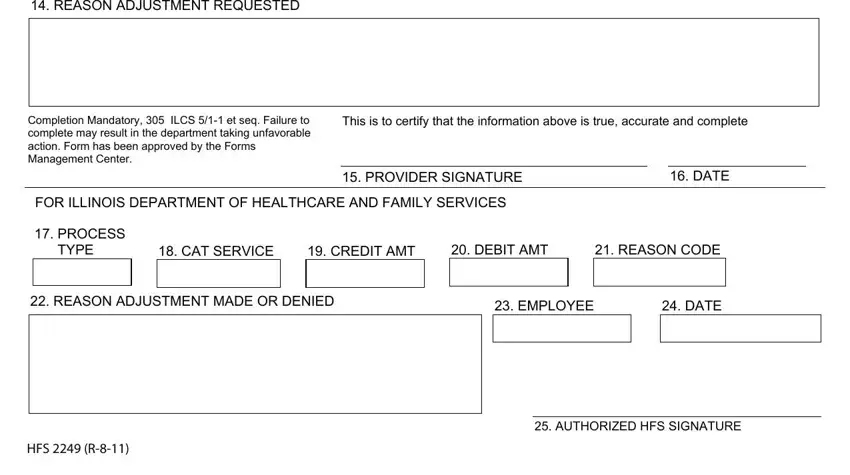
You can potentially make errors when completing the This is to certify that the, thus make sure that you take a second look before you finalize the form.
Step 3: Be certain that the information is accurate and just click "Done" to progress further. After registering a7-day free trial account at FormsPal, you will be able to download hfs 2249 form or send it through email right away. The PDF document will also be accessible through your personal account page with all of your changes. FormsPal offers safe document tools without personal data recording or distributing. Rest assured that your data is in good hands with us!