
Dealing with PDF documents online is very easy using our PDF tool. Anyone can fill in Form Hhs 758 here with no trouble. Our team is devoted to providing you the absolute best experience with our tool by constantly releasing new capabilities and improvements. With these updates, using our editor becomes better than ever! With some easy steps, you can start your PDF journey:
Step 1: First, access the tool by clicking the "Get Form Button" at the top of this page.
Step 2: Using this advanced PDF file editor, you are able to accomplish more than just complete blank form fields. Try each of the features and make your forms appear great with customized text added, or optimize the original content to excellence - all backed up by an ability to incorporate your personal pictures and sign the document off.
For you to finalize this PDF document, make sure you type in the necessary information in each blank field:
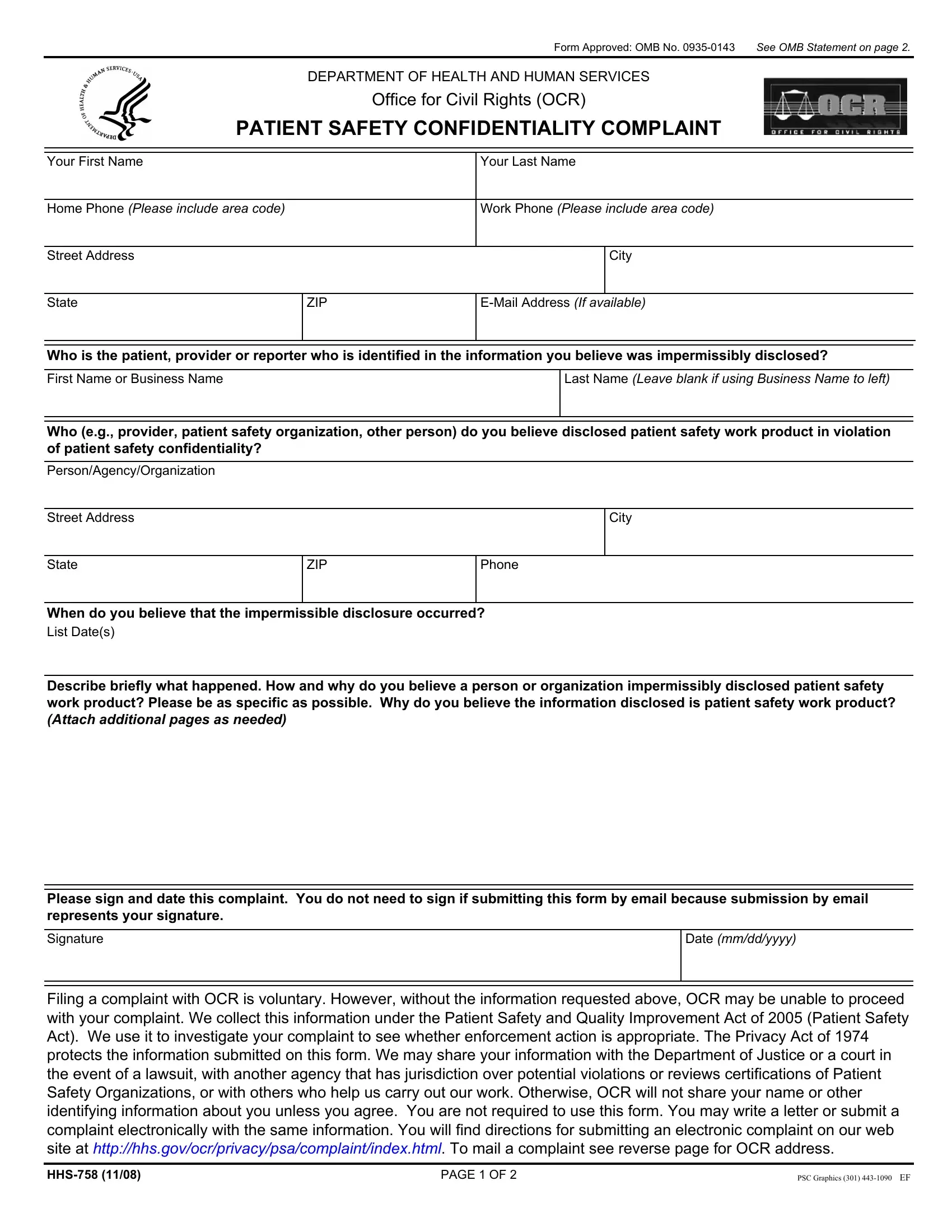
1. While filling out the Form Hhs 758, be sure to complete all important blanks within its relevant area. This will help hasten the process, making it possible for your details to be processed promptly and correctly.
2. After this part is done, go on to type in the applicable information in all these - Describe briefly what happened How, Please sign and date this, Signature, Date mmddyyyy, and Filing a complaint with OCR is.
3. Completing Do you need special accommodations, Braille, Large print, Cassette tape, Computer diskette, Electronic Mail, TDD, Sign language interpreter Specify, Foreign language interpreter, Other Specify, To help us better serve you answer, HOW DID YOU LEARN ABOUT THE OFFICE, HHS Website Internet Search, Family Friend Associate, and Religious Community Org is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Regarding Large print and Computer diskette, ensure that you do everything right in this current part. Both these are the most significant ones in this document.
4. To go ahead, this next section requires filling out several form blanks. Examples of these are State, ZIP, EMail Address If available, Have you filed your complaint, Person Agency Organization, Dates Filed, Case Numbers If known, To mail a complaint please type or, Office for Civil Rights, Department of Health and Human, Attn Patient Safety Act, Independence Ave SW Rm F, Washington DC, TDD FAX, and To submit an electronic complaint, which you'll find crucial to continuing with this particular process.
Step 3: Ensure that your details are right and then click "Done" to finish the task. Acquire your Form Hhs 758 once you join for a free trial. Instantly gain access to the pdf form from your FormsPal cabinet, along with any edits and changes being all preserved! At FormsPal, we endeavor to be sure that all your information is maintained protected.