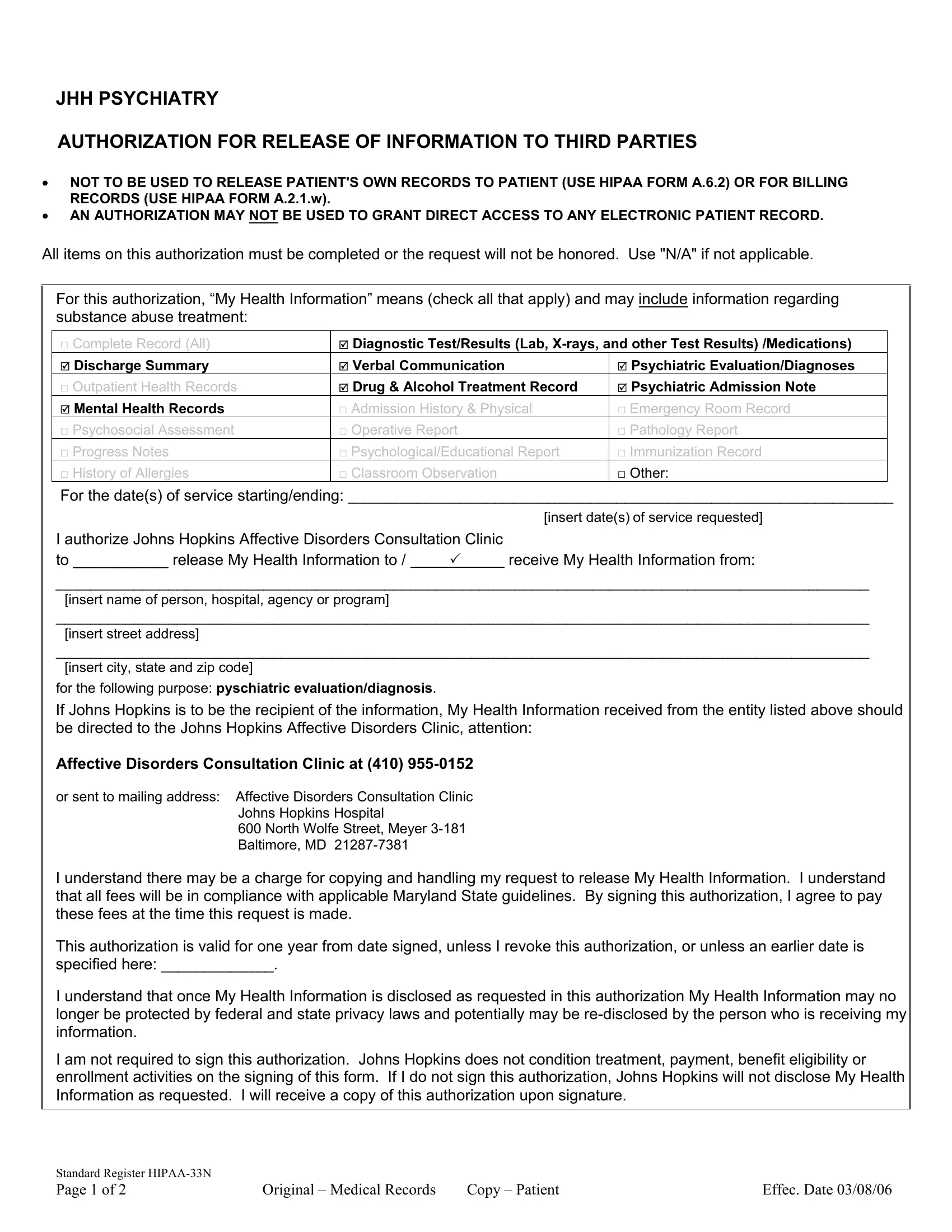
In the realm of medical records and patient privacy, the HIPAA 33N form serves as a critical tool for authorizing the release of specific health information to third parties, distinct from granting access to a patient's own records or billing information. This form, specifically utilized within the Johns Hopkins Affective Disorders Consultation Clinic, delineates a structured process to ensure that a patient or their legally authorized representative can allow or restrict the sharing of sensitive health data. The form comprehensively covers various types of information that may be shared, including but not limited to psychiatric evaluations, drug and alcohol treatment records, and mental health records, catering to a wide array of medical disclosure needs. It stresses the importance of explicit consent by requiring the completion of all items for the authorization to be valid, thereby upholding the fundamental tenets of patient autonomy and privacy. Additionally, the form outlines the potential for associated fees, in compliance with Maryland State guidelines, highlighting the patient’s responsibility for any costs incurred in the process. Moreover, it acknowledges the finite nature of this authorization, which is subject to revocation by the patient at any time, albeit under specified conditions to ensure the request’s validity. The HIPAA 33N form encapsulates the nuanced balance between the necessity for information sharing in healthcare settings and the imperative to protect patient privacy under state and federal laws.
| Question | Answer |
|---|---|
| Form Name | Form Hipaa 33N |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Maryland, Hopkins, HIPAA, johns hopkins hospital medical records |
