In the realm of medical records and patient privacy, the HIPAA 33N form serves as a critical tool for authorizing the release of specific health information to third parties, distinct from granting access to a patient's own records or billing information. This form, specifically utilized within the Johns Hopkins Affective Disorders Consultation Clinic, delineates a structured process to ensure that a patient or their legally authorized representative can allow or restrict the sharing of sensitive health data. The form comprehensively covers various types of information that may be shared, including but not limited to psychiatric evaluations, drug and alcohol treatment records, and mental health records, catering to a wide array of medical disclosure needs. It stresses the importance of explicit consent by requiring the completion of all items for the authorization to be valid, thereby upholding the fundamental tenets of patient autonomy and privacy. Additionally, the form outlines the potential for associated fees, in compliance with Maryland State guidelines, highlighting the patient’s responsibility for any costs incurred in the process. Moreover, it acknowledges the finite nature of this authorization, which is subject to revocation by the patient at any time, albeit under specified conditions to ensure the request’s validity. The HIPAA 33N form encapsulates the nuanced balance between the necessity for information sharing in healthcare settings and the imperative to protect patient privacy under state and federal laws.
| Question | Answer |
|---|---|
| Form Name | Form Hipaa 33N |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Maryland, Hopkins, HIPAA, johns hopkins hospital medical records |
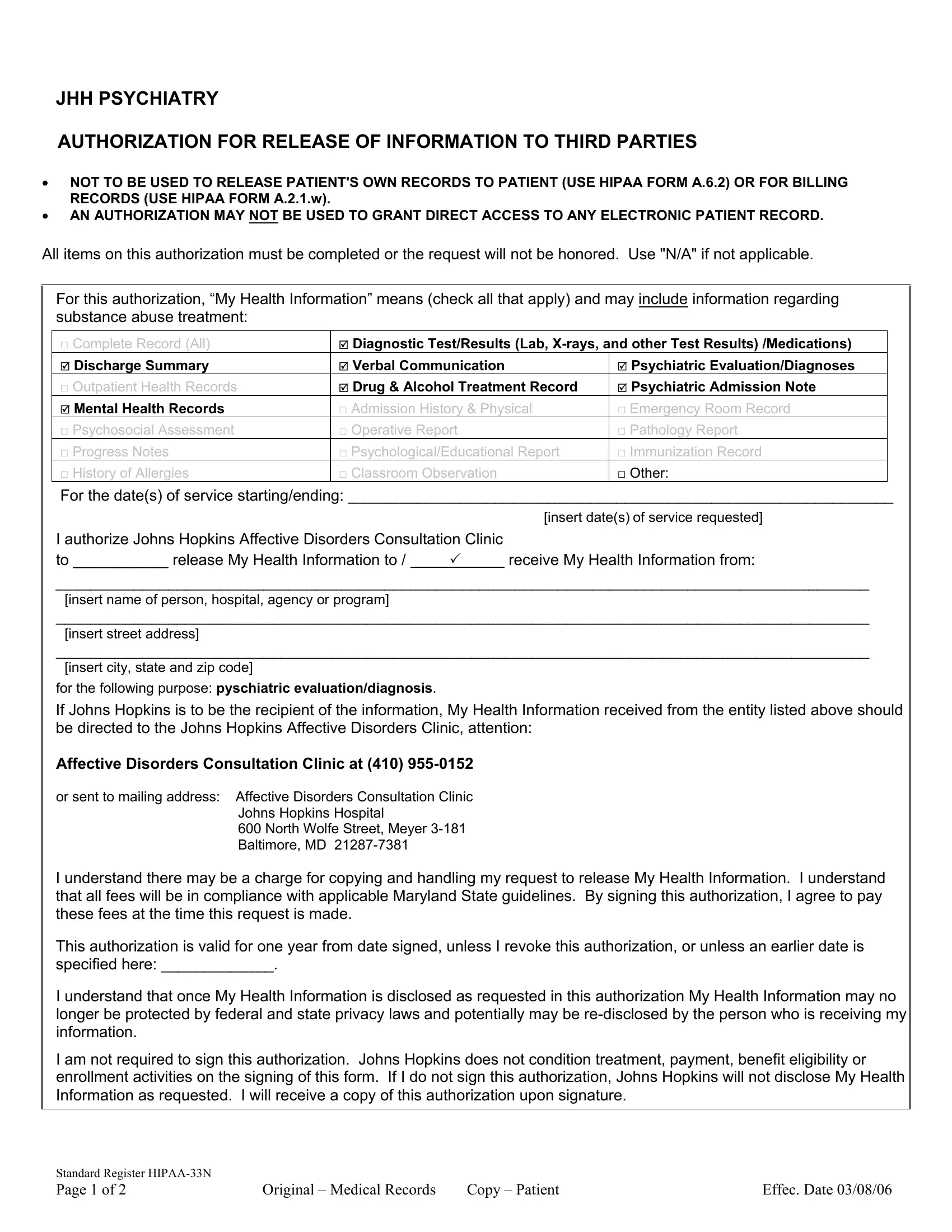
JHH PSYCHIATRY
AUTHORIZATION FOR RELEASE OF INFORMATION TO THIRD PARTIES
•NOT TO BE USED TO RELEASE PATIENT'S OWN RECORDS TO PATIENT (USE HIPAA FORM A.6.2) OR FOR BILLING RECORDS (USE HIPAA FORM A.2.1.w).
•AN AUTHORIZATION MAY NOT BE USED TO GRANT DIRECT ACCESS TO ANY ELECTRONIC PATIENT RECORD.
All items on this authorization must be completed or the request will not be honored. Use "N/A" if not applicable.
For this authorization, “My Health Information” means (check all that apply) and may include information regarding substance abuse treatment:
□ Complete Record (All) |
5 Diagnostic Test/Results (Lab, |
|
5 Discharge Summary |
5 Verbal Communication |
5 Psychiatric Evaluation/Diagnoses |
□ Outpatient Health Records |
5 Drug & Alcohol Treatment Record |
5 Psychiatric Admission Note |
5 Mental Health Records |
□ Admission History & Physical |
□ Emergency Room Record |
□ Psychosocial Assessment |
□ Operative Report |
□ Pathology Report |
□ Progress Notes |
□ Psychological/Educational Report |
□ Immunization Record |
□ History of Allergies |
□ Classroom Observation |
□ Other: |
For the date(s) of service starting/ending: _______________________________________________________________
|
|
[insert date(s) of service requested] |
I authorize Johns Hopkins Affective Disorders Consultation Clinic |
|
|
to ___________ release My Health Information to / |
|
receive My Health Information from: |
______________________________________________________________________________________________
[insert name of person, hospital, agency or program]
______________________________________________________________________________________________
[insert street address]
______________________________________________________________________________________________
[insert city, state and zip code]
for the following purpose: pyschiatric evaluation/diagnosis.
If Johns Hopkins is to be the recipient of the information, My Health Information received from the entity listed above should be directed to the Johns Hopkins Affective Disorders Clinic, attention:
Affective Disorders Consultation Clinic at (410)
or sent to mailing address: Affective Disorders Consultation Clinic Johns Hopkins Hospital
600 North Wolfe Street, Meyer
I understand there may be a charge for copying and handling my request to release My Health Information. I understand that all fees will be in compliance with applicable Maryland State guidelines. By signing this authorization, I agree to pay these fees at the time this request is made.
This authorization is valid for one year from date signed, unless I revoke this authorization, or unless an earlier date is specified here: _____________.
I understand that once My Health Information is disclosed as requested in this authorization My Health Information may no longer be protected by federal and state privacy laws and potentially may be
I am not required to sign this authorization. Johns Hopkins does not condition treatment, payment, benefit eligibility or enrollment activities on the signing of this form. If I do not sign this authorization, Johns Hopkins will not disclose My Health Information as requested. I will receive a copy of this authorization upon signature.
Standard Register |
|
|
|
Page 1 of 2 |
Original – Medical Records |
Copy – Patient |
Effec. Date 03/08/06 |
Patient Name:
|
(first) |
(m. initial) |
(last) |
|||
Signature: |
|
|
|
Date: |
|
|
Address: |
|
|
|
|
|
|
(street address) |
|
|
(apt. number) |
|
||
|
|
|
|
|||
|
|
|
|
|
||
|
(city) |
(state) |
(zip code) |
|||
Phone: |
|
|
|
|
|
|
(area code) |
|
(home phone number) |
|
|||
|
|
|
||||
Birth Date: |
|
|
Medical Record #: |
|
||
As the healthcare agent/court appointed guardian/parent/informal kinship care relative, I,
(circle one of the above)
________________________________________ confirm that I am the representative for the patient as circled
above.
(insert your name)
Representative’s Signature:
Address: ______________________________________________________ Phone: _______________________
If you are the healthcare agent, court appointed guardian, or relative providing informal kinship care, please attach proof of your authority to act on behalf of the patient.
By signing this authorization, I understand that medical records released may contain information related to HIV status, AIDS, sexually transmitted diseases, mental health, drug and alcohol abuse, etc. I understand that release of psychotherapy notes requires an additional authorization.
Notice to the Individual signing this form: The confidentiality of information concerning alcohol or drug abuse treatment is protected by federal law (Federal Regulation 42 CFR Part 2) and prohibits the recipient from further disclosing this information except with specific written authorization of the person to whom it pertains. A general authorization for release of medical or other information is not sufficient for that purpose.
I may revoke this authorization by mailing or faxing my written request along with a copy of the original authorization to the Health Care Provider identified above that provided the health information.
If I am unable to provide a copy of the original authorization with my request to revoke, I will provide the following information.
•Date of the authorization,
•Name,
•Address,
•Phone number,
•Medical record number,
•Date of birth,
•Purpose of authorization,
•A description of the health information covered by the authorization,
•The person or entity authorized to use the data.
If the form was signed by my representative, the request will also include:
•The representative’s name,
•Relationship,
•Address and
•Phone number.
I understand that if I am unable to provide all of the above information, Johns Hopkins may not be able to honor my revocation request.
Standard Register |
|
|
|
Page 2 of 2 |
Original – Medical Records |
Copy – Patient |
Effec. Date 03/08/06 |