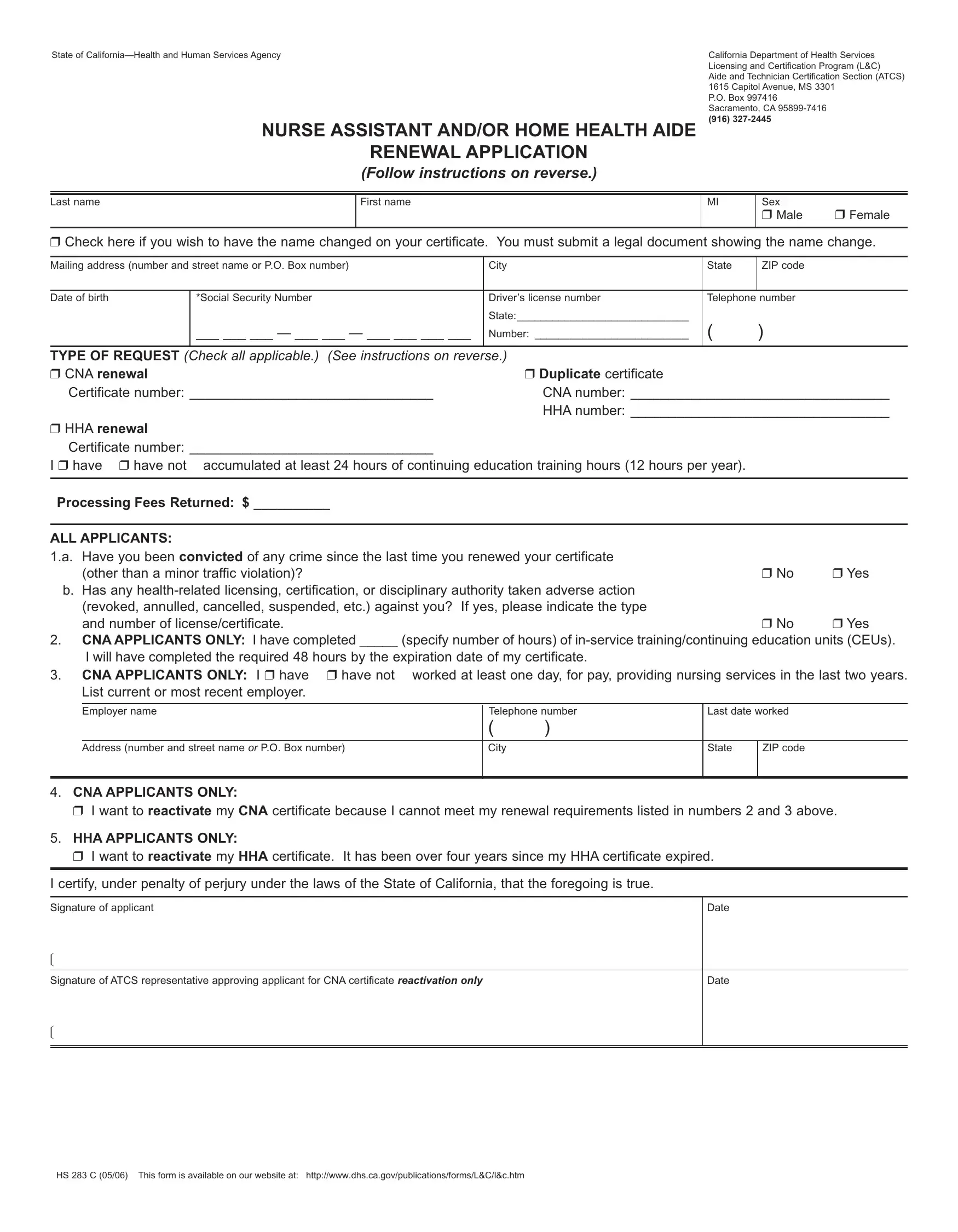
Navigating the landscape of renewing a certification in the healthcare field can be complex, and for those holding a nurse assistant and/or home health aide certificate in California, understanding the details of the HS 283 C form is crucial. Issued by the California Department of Health Services, specifically under its Licensing and Certification Program, this form serves a dual purpose for both renewal and reactivation of certificates. Applicants are presented with sections to fill out personal details, detail their work experience, continuing education hours, and any criminal convictions or licensing disciplinary actions since their last renewal. Additionally, the form outlines requirements for both nurse assistant (CNA) and home health aide (HHA) renewals, including the necessity of having completed certain hours of in-service training and having provided nursing-related services within a specified timeframe. For those unable to meet the renewal criteria, a pathway for reactivation without re-training is also provided, provided the certificate has not been expired for over the set period. Moreover, the form encompasses privacy statements concerning the collection and use of social security numbers, underlining its mandatory disclosure for certification purposes. As the form is available online, it signifies a step towards easing the administrative burdens faced by healthcare professionals, ensuring they can focus more on their critical roles in patient care.
| Question | Answer |
|---|---|
| Form Name | Form Hs 283 C |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CNA, 12-months, HHA, reactivation |
State of |
|
California Department of Health Services |
||||
|
|
|
|
Licensing and Certification Program (L&C) |
||
|
|
|
|
Aide and Technician Certification Section (ATCS) |
||
|
|
|
|
1615 Capitol Avenue, MS 3301 |
||
|
|
|
|
P.O. Box 997416 |
|
|
|
|
|
|
Sacramento, |
|
|
|
NURSE ASSISTANT AND/OR HOME HEALTH AIDE |
(916) |
|
|||
|
|
|
|
|||
|
|
RENEWALAPPLICATION |
|
|
|
|
|
|
(Follow instructions on reverse.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last name |
|
First name |
|
MI |
Sex |
|
|
|
|
|
|
❒ Male |
❒ Female |
|
|
|
|
|
|
|
❒ Check here if you wish to have the name changed on your certificate. You must submit a legal document showing the name change. |
||||||
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box number) |
City |
State |
ZIPcode |
|
||
|
|
|
|
|
|
|
Date of birth |
*Social Security Number |
Driver’s license number |
Telephone number |
|
||
|
|
|
State:_____________________________ |
|
|
|
|
___ ___ ___ — ___ ___ — ___ ___ ___ ___ |
Number: __________________________ |
( |
) |
|
|
|
|
|
|
|
|
|
TYPE OF REQUEST (Check all applicable.) (See instructions on reverse.) |
|
|
|
|||
❒ CNA renewal |
|
|
❒ Duplicate certificate |
|
|
|
Certificate number: ________________________________ |
CNAnumber: __________________________________ |
|||||
|
|
|
HHAnumber: __________________________________ |
|||
❒ HHA renewal |
|
|
|
|
|
|
Certificate number: ________________________________
I ❒ have ❒ have not accumulated at least 24 hours of continuing education training hours (12 hours per year).
PROCESSING FEES Returned: $ __________
ALLAPPLICANTS: |
|
|
1.a. Have you been convicted of any crime since the last time you renewed your certificate |
|
|
(other than a minor traffic violation)? |
❒ No |
❒ Yes |
b. Has any |
|
|
(revoked, annulled, cancelled, suspended, etc.) against you? If yes, please indicate the type |
|
|
and number of license/certificate. |
❒ No |
❒ Yes |
2.CNAAPPLICANTSONLY: I have completed _____ (specify number of hours) of
3. CNAAPPLICANTS ONLY: I ❒ have ❒ have not |
worked at least one day, for pay, providing nursing services in the last two years. |
|||||
List current or most recent employer. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer name |
|
Telephone number |
Last date worked |
||
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
Address (number and street name or P.O. Box number) |
|
City |
|
State |
ZIPcode |
|
|
|
|
|
|
|
4.CNAAPPLICANTS ONLY:
❒I want to reactivate my CNA certificate because I cannot meet my renewal requirements listed in numbers 2 and 3 above.
5.HHAAPPLICANTS ONLY:
❒I want to reactivate my HHA certificate. It has been over four years since my HHAcertificate expired.
I certify, under penalty of perjury under the laws of the State of California, that the foregoing is true.
Signature of applicant |
Date |
|
|
Signature of ATCS representative approving applicant for CNAcertificate reactivation only |
Date |
HS 283C (05/06) This form is available on our website at: http://www.dhs.ca.gov/publications/forms/L&C/l&c.htm
INSTRUCTIONS
A.CNA RENEWALS
You may renew your certificate any time within two years after the expiration date of your certificate if the following applies:
1.You submit a completed application to ATCS;
2.You have been fingerprinted for Certified Nurse Assistant (CNA), Home Health Aide (HHA), Intermediate Care Facility – Developmentally Disabled
3.You provided nursing or
4.You presently or by the time your certificate expires, completed 48 hours of
B.HHA RENEWALS
You may renew your certificate any time within four years after the expiration date of your certificate if:
1.You presently or by the time your certificate expires, completed 24 hours or
C.CNA REACTIVATION
If you are unable to meet the renewal requirements and your certificate has not expired over two years, you may submit this completed application for REACTIVATION without needing
If you are qualified, ATCS will approve your application for the competency evaluation and will send you information about taking the competency evaluation (i.e. testing). You will not receive certification until the testing vendor (American Red Cross and Nurse Assistant Training & Assessment Program) notifies ATCS that you passed the competency evaluation and you obtain criminal clearance from the Department of Justice.
Certificate Holders with both nurse assistant and home health aide certificates shall renew their certificates at the same time on one application.
INFORMATION COLLECTION AND ACCESS: PRIVACYSTATEMENT
*Social Security Number Disclosure: Pursuant to Section 666(a)(13) of Title 42 of the United States Code and California Family Code, Section17520, subdivision(d), the California Department of Health Services (CDHS) is required to collect social security numbers from all applicants for nursing assistant certificates, home health aide certificates, hemodialysis technician certificates or nursing home administrator licenses. Disclosure of your social security number is mandatory for purposes of establishing, modifying, or enforcing child support orders upon request by the Health Integrity and Protection Data Bank as required by 45 CFR §61.1 etseq. Failure to provide your social security number will result in the return of your application. Your social security number will be used by CHDS for internal identification, and may be used to verify information on your application, to verify certification with another state’s certification authority, for exam identification, for identification purposes in national disciplinary databases or as the basis of a disciplinary action against you.
Aforementioned requirements are based on Health & Safety Code commencing with §1337 through 1338.5, 1725 through 1742 and 42 Code of Federal Regulations, Chapter IV, commencing wtih §483.13, 483.156, and 483.75, and Title 22 California Code of Regulations, commencing with §71801.
HS 283C (05/06) This form is available on our website at: http://www.dhs.ca.gov/publications/forms/L&C/l&c.htm |
OSP06 96238 |