

Working with PDF documents online is certainly easy with our PDF tool. You can fill out Form Hs 283 F here within minutes. To make our editor better and simpler to work with, we continuously implement new features, taking into consideration suggestions from our users. With some simple steps, you can begin your PDF editing:
Step 1: Just press the "Get Form Button" in the top section of this page to get into our pdf editing tool. This way, you'll find everything that is needed to work with your file.
Step 2: The tool offers the opportunity to customize your PDF document in a range of ways. Change it by writing your own text, adjust what's already in the file, and add a signature - all at your fingertips!
This document requires particular information to be filled in, therefore be sure you take some time to provide what is requested:
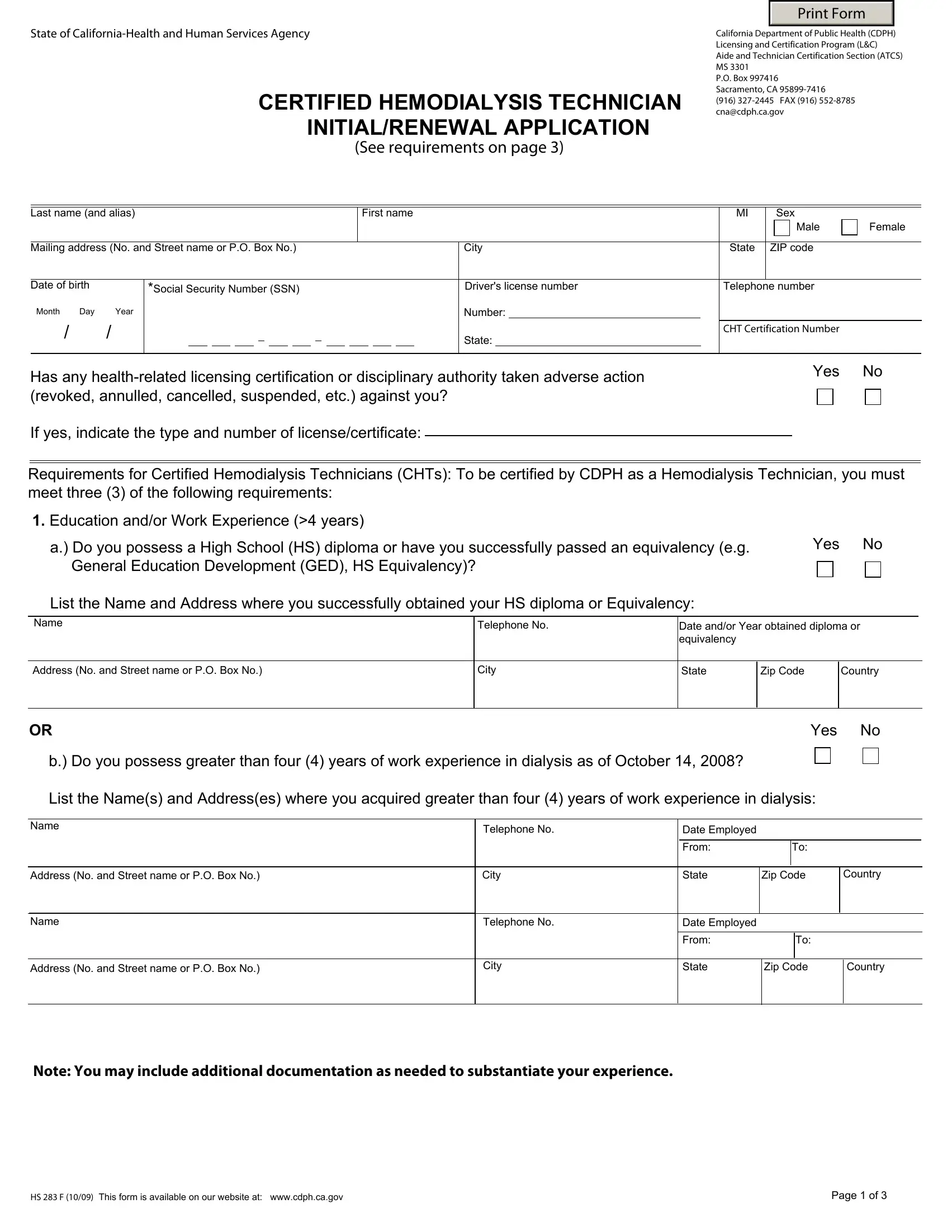
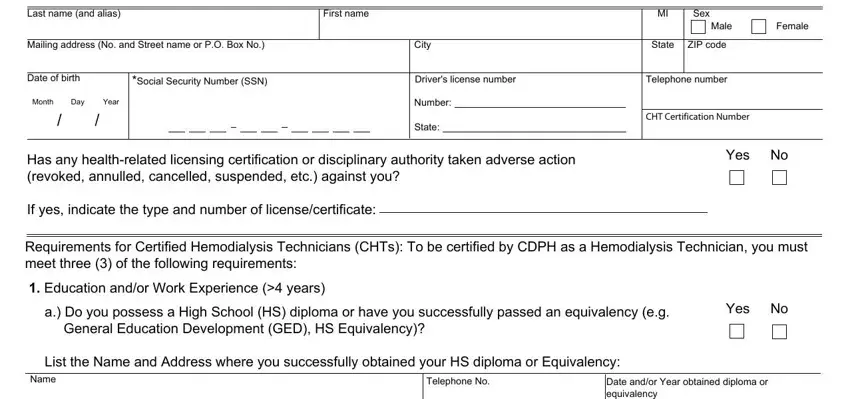
1. To get started, when filling in the Form Hs 283 F, start in the part that contains the next blank fields:
2. After filling in the last section, go to the next step and enter all required details in all these blank fields - Address No and Street name or PO, City, State, Zip Code, Country, Yes, b Do you possess greater than four, Name, Telephone No, Date Employed, Address No and Street name or PO, City, From, State, and Zip Code.
3. In this particular stage, take a look at Name, Telephone No, Date Program Completed, Training Program Provider No, Address No and Street name or PO, City, State, Zip Code, Country, Print Name of Registered Nurse RN, Signature of RN Trainer, Date, b Equivalent Experience in Lieu of, Date employed at Dialysis Clinic, and Telephone No. All these are required to be filled in with highest accuracy.
Always be extremely mindful while completing City and Country, because this is the part where most users make mistakes.
4. The subsequent paragraph needs your input in the following places: a Did you successfully pass a, Medicare and Medicaid Services CMS, If yes indicate the name of, Yes, Yes, Name of Test or Examination, Telephone No, Date Passed the Test or Examination, Independent Examiners Provider No, Address No and Street name or PO, City, State, Zip Code, Country, and Print Name of Proctor who. Always give all requested info to move onward.
Step 3: Right after rereading the fields, click "Done" and you are good to go! Grab the Form Hs 283 F the instant you subscribe to a free trial. Immediately view the pdf file within your personal cabinet, together with any edits and adjustments being automatically kept! When you use FormsPal, you can certainly fill out documents without being concerned about data breaches or entries being shared. Our secure software makes sure that your private information is stored safe.