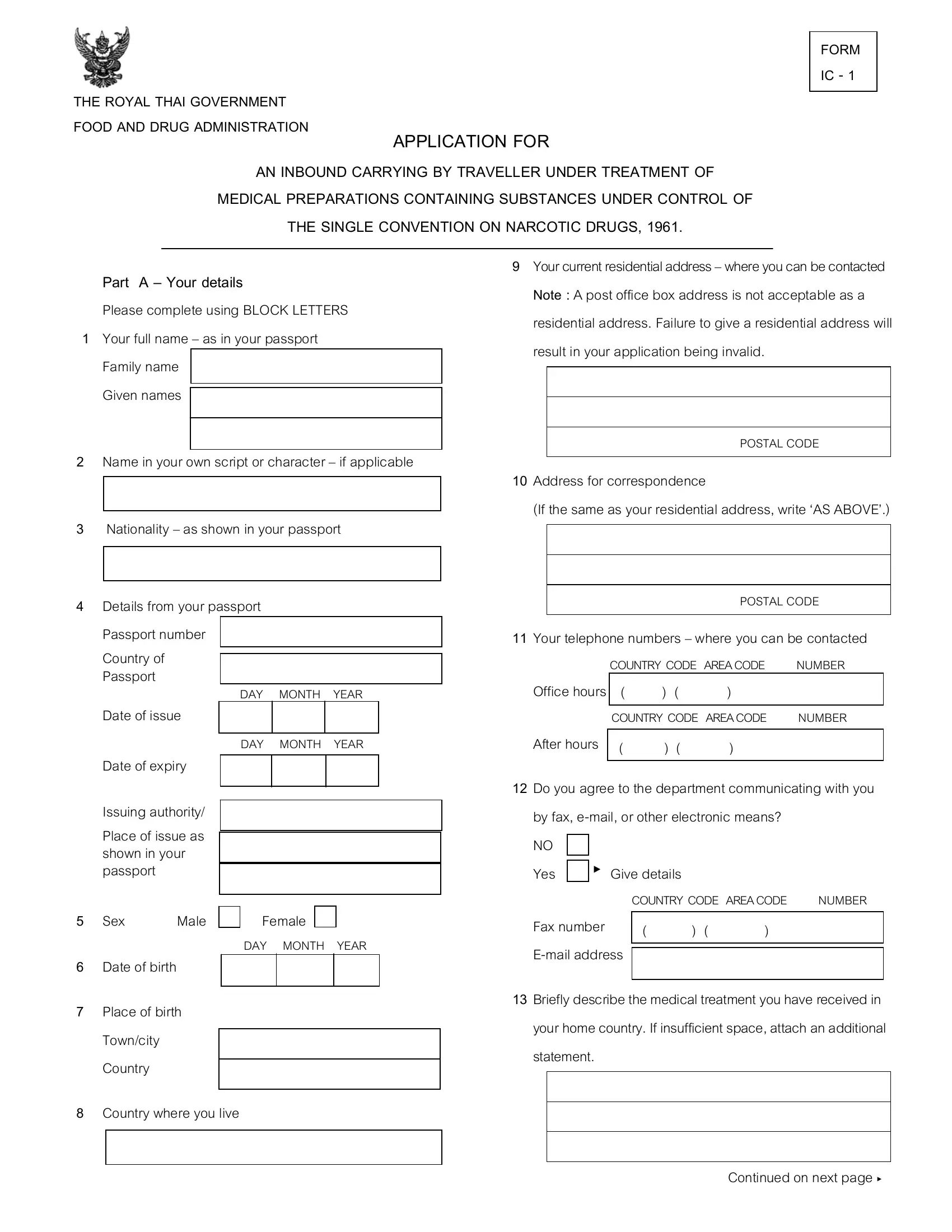
Travelers undergoing treatment who wish to carry medications containing substances regulated under the Single Convention on Narcotic Drugs, 1961, into Thailand must navigate a specific bureaucratic process. This process is crystallized in the form known as IC-1, mandated by the Royal Thai Government Food and Drug Administration. Essential for those under medical treatment wishing to carry necessary medications across borders, the form serves as an application to legally transport drugs that would otherwise be tightly controlled. Applicants are required to fill in comprehensive details starting from personal information as found in their passport, including full name and nationality, to more specific data such as their residential address and contact information. The form does not accept post office boxes as a valid residential address, emphasizing the government's strict adherence to verifiable details. Moreover, it extends into a detailed declaration regarding the applicant's medical treatment, the medical professional overseeing their care, and the specific medications prescribed – all of which are under the scrutiny of international narcotics control. The I-1 form further probes into the applicant's travel itinerary, questioning about relatives in Thailand, and inquires if the applicant’s medical condition might incur additional medical expenses during their stay. This thorough application process underscores the careful balance Thailand seeks to maintain between upholding international drug control standards and accommodating the medical needs of international travelers.
| Question | Answer |
|---|---|
| Form Name | Form Ic 1 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form for ic 12 26 4 6, ic 1 form medication thailand, form ic 1, form ic 2 |
THE ROYAL THAI GOVERNMENT FOOD AND DRUG ADMINISTRATION
FORM
IC - 1
APPLICATION FOR
AN INBOUND CARRYING BY TRAVELLER UNDER TREATMENT OF
MEDICAL PREPARATIONS CONTAINING SUBSTANCES UNDER CONTROL OF
THE SINGLE CONVENTION ON NARCOTIC DRUGS, 1961.
PART A – YOUR DETAILS
Please complete using BLOCK LETTERS
1Your full name – as in your passport
Family name
Given names
2Name in your own script or character – if applicable
3Nationality – as shown in your passport
4Details from your passport
Passport number
Country of
Passport
DAY MONTH YEAR
Date of issue
DAY MONTH YEAR
Date of expiry
Issuing authority/
Place of issue as shown in your passport
9Your current residential address – where you can be contacted NOTE : A post office box address is not acceptable as a residential address. Failure to give a residential address will result in your application being invalid.
POSTAL CODE
10Address for correspondence
(If the same as your residential address, write ‘AS ABOVE’.)
POSTAL CODE
11Your telephone numbers – where you can be contacted
COUNTRY CODE AREACODE NUMBER
Office hours |
( |
) |
( |
) |
|
|
|
|
|||
|
COUNTRY CODE AREACODE |
NUMBER |
|||
|
|
|
|
|
|
After hours |
( |
) |
( |
) |
|
|
|
|
|
|
|
12Do you agree to the department communicating with you
by fax,
NO
Yes ►
COUNTRY CODE AREACODE |
NUMBER |
5 Sex |
Male |
6Date of birth
7Place of birth Town/city Country
Female
DAY MONTH YEAR
Fax number |
( |
) ( |
) |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13Briefly describe the medical treatment you have received in your home country. If insufficient space, attach an additional statement.
8Country where you live
Continued on next page ►
14Give details of the doctor in your home country who provided you with medical treatment.
Name and Licence number of doctor.
Address
POSTAL CODE
15Give the expected date of arrival and departure from Thailand and details of arrangement for your continued
care in your home country.
DAY MONTH YEAR
Date of arrival
DAY MONTH YEAR
Date of departure Details of arrangement. If insufficient space, attach an additional statement
16Give details of the medical preparations containing substances under control of the Single Convention on Narcotic Drugs, 1961, which the doctor in your home country arranged for you during your stay in Thailand. (For amounts not exceeding 30 days of treatment)
Details of medical preparations (Trade name, generic name , strength and quantity). If insufficient space, attach an additional statement.
17Give details of your itineraries Embarkation Port
Carrier / Flight number
Disembarkation Port
Carrier / Flight number
18Do you have any relatives or friends in Thailand ?
NO |
|
Yes |
► Give all relevant details |
Name of person
Relationship Permanent resident of Thailand ?
NO Yes Address
POSTAL CODE
19During your proposed stay in Thailand, do you have or expect to incur medical costs or require treatment or medical follow up for your medical condition?
NO |
|
Yes |
► Please provide full details. |
If insufficient space, attach an additional statement.
PART B – DECLARATION
20Applicant
•I declare that the information on this form is complete, correct and
•I will abide by the condition imposed on the permit
granted.
Signature of applicant
DAY MONTH YEAR
Date