


Any time you wish to fill out Form Ic1, you won't have to install any software - simply try our online PDF editor. In order to make our editor better and less complicated to work with, we continuously design new features, with our users' feedback in mind. This is what you will have to do to start:
Step 1: Click on the "Get Form" button above. It's going to open up our pdf editor so that you can begin filling out your form.
Step 2: As soon as you launch the tool, you will find the document ready to be filled out. In addition to filling out different blanks, you can also do many other things with the file, specifically writing custom text, editing the initial textual content, inserting images, signing the document, and much more.
So as to finalize this PDF form, ensure you provide the right details in every single field:
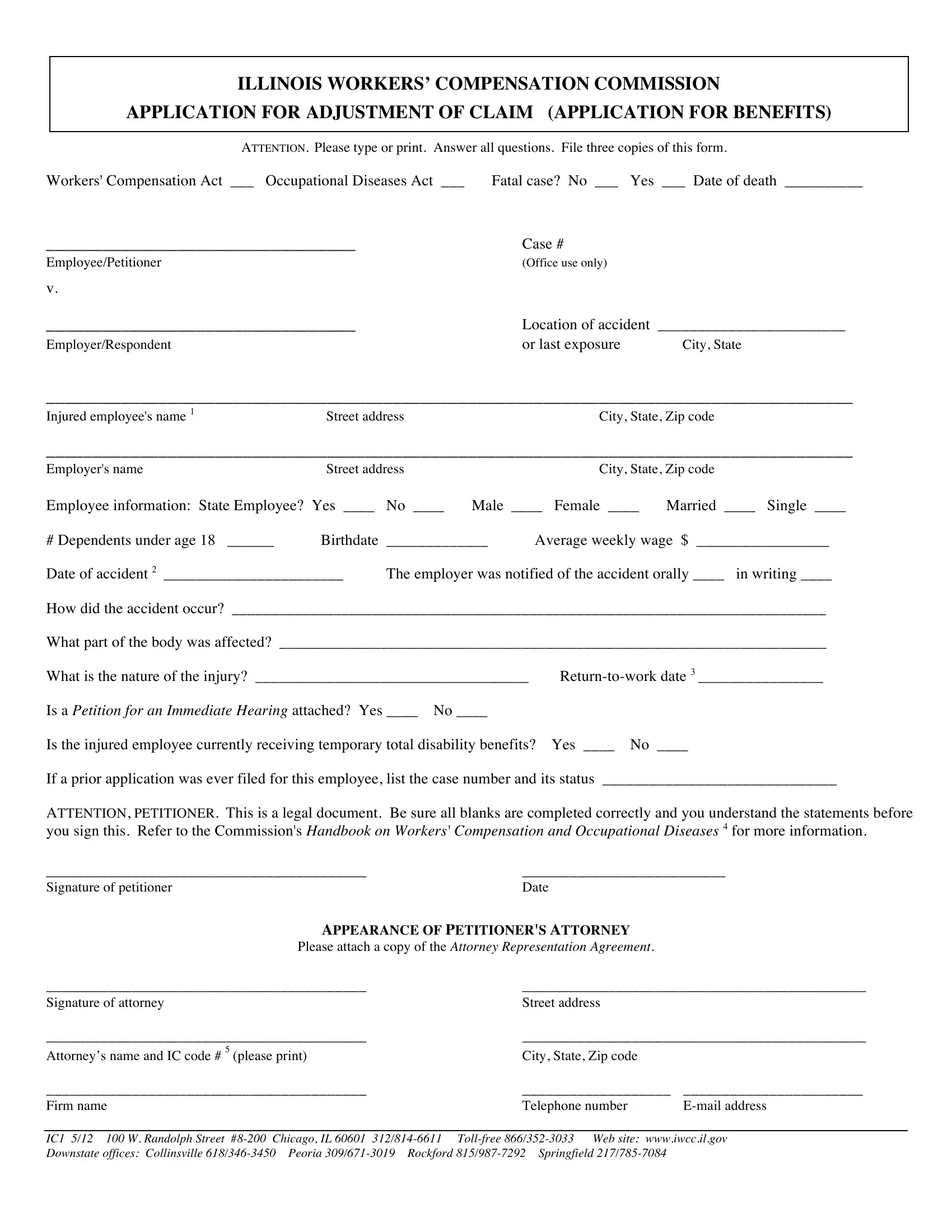
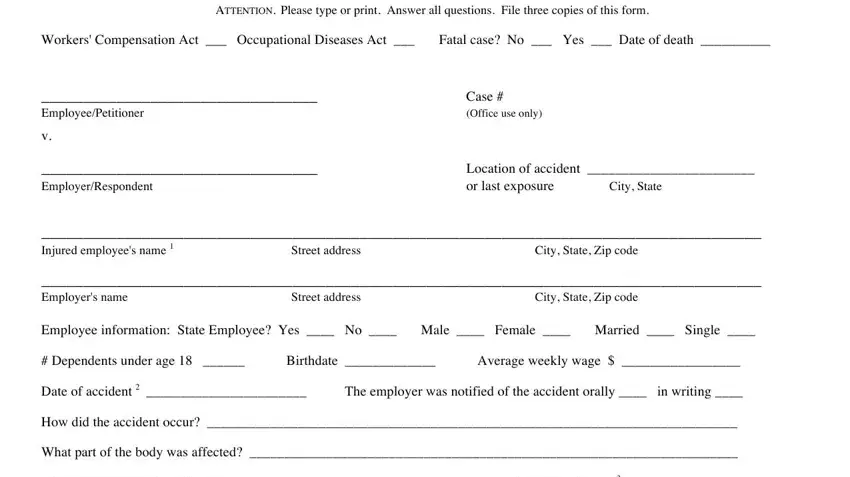
1. When completing the Form Ic1, be sure to incorporate all necessary fields in its associated form section. This will help to hasten the work, allowing your information to be handled quickly and appropriately.
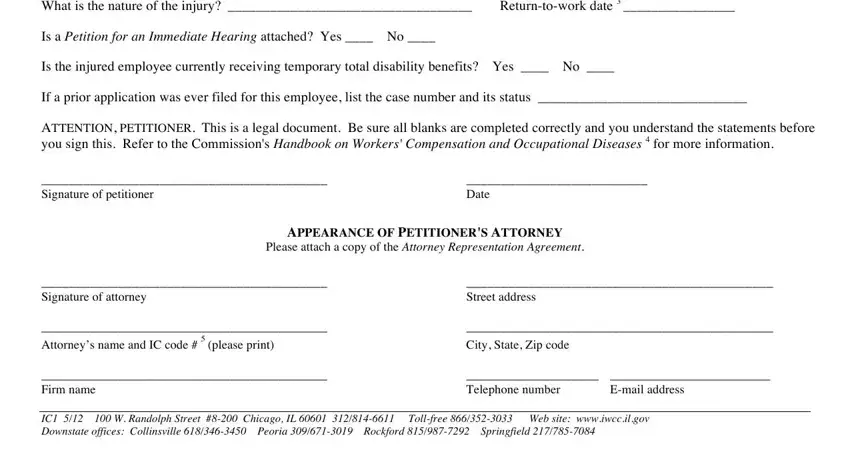
2. Once your current task is complete, take the next step – fill out all of these fields - v EmployerRespondent Injured, Date, APPEARANCE OF PETITIONERS ATTORNEY, Please attach a copy of the, Signature of attorney Attorneys, please print, City State Zip code, Telephone number, Email address, and Street address with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. This third step is going to be straightforward - complete all the form fields in I affirm that I delivered to complete this part.
Those who work with this PDF frequently make errors when filling out I affirm that I delivered in this area. Make sure you go over everything you type in right here.
Step 3: Check that your details are correct and then simply click "Done" to finish the task. Grab the Form Ic1 when you register here for a free trial. Instantly access the pdf from your personal account page, with any edits and adjustments all saved! When you work with FormsPal, it is simple to complete forms without being concerned about information leaks or records getting shared. Our protected platform makes sure that your personal information is kept safe.