Instructions for Form IMS-01 (Revised 01/28/2019)
User ID and System Access Request Form Instructions
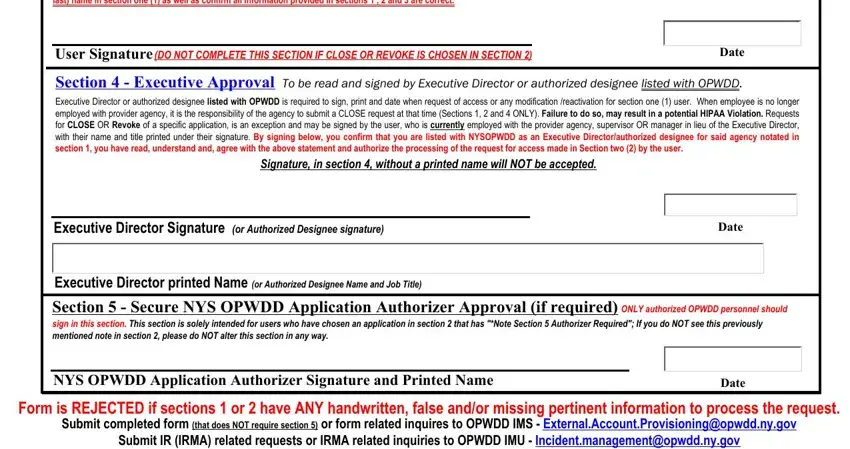
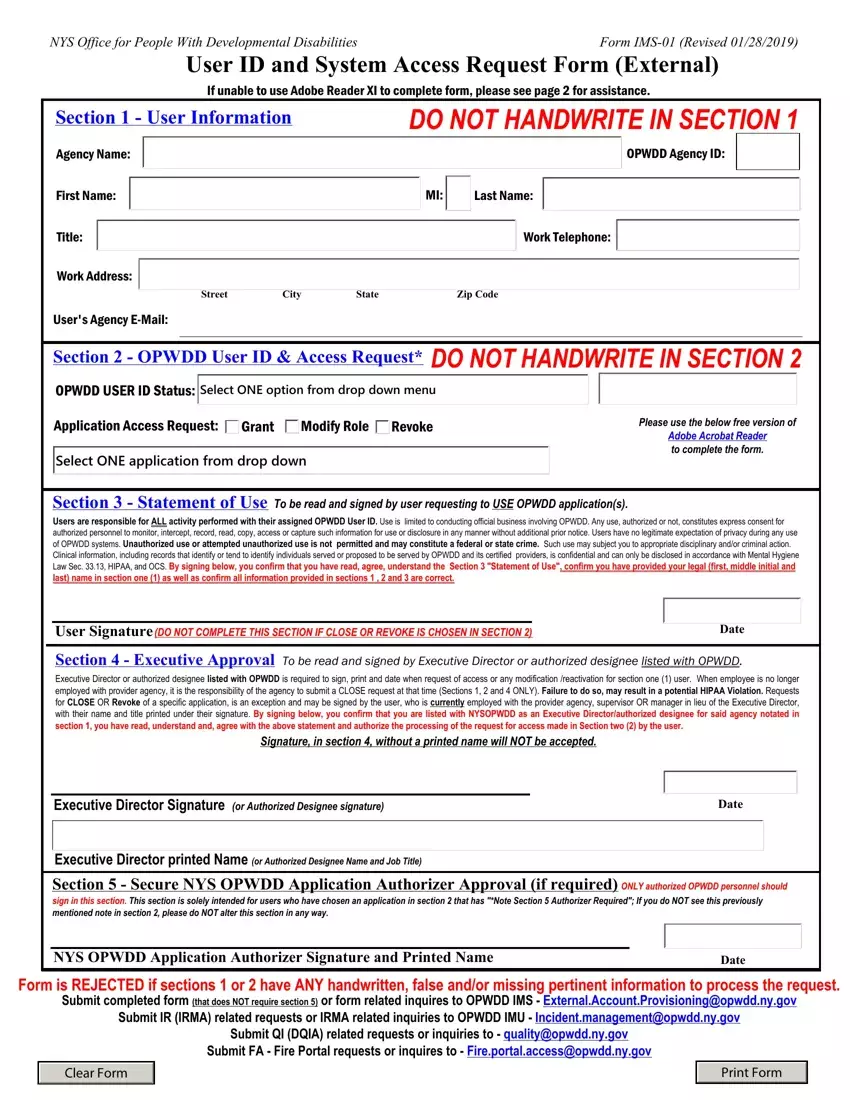
Form is REJECTED if sections 1 or 2 have ANY handwritten, false or missing pertinent information to process the request.
Staff who have NOT officially started working at the agency should NOT request access to the OPWDD systems.
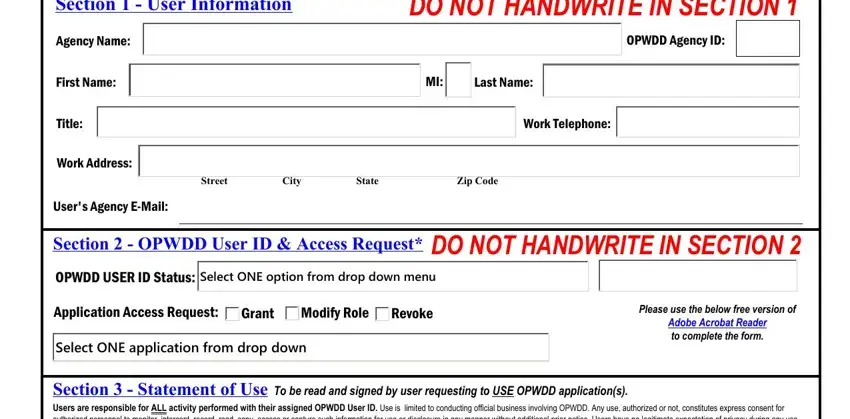
Section 1 - User Information - Do NOT handwrite ANY information.
Please type ALL information requested, do NOT leave any box blank if requesting to use secure OPWDD application(s).
Provide LEGAL First name, middle initial and last name.
If no LEGAL middle name: type an “X”; user must submit their form and confirm they do not legally have a middle name OR middle name begins with an “X”, within the body of the e-mail submission.
Section 2 - OPWDD User ID & Access Request - Do NOT handwrite ANY information.
Part 1 - Select ONE option from the OPWDD User ID Status drop down menu.
OPWDD User ID - User has a User ID with Agency/agency ID provided in section 1. Go to part 2.
I do NOT have an OPWDD User ID* - User does not have an OPWDD User ID in system. Go to part 2.
Additional OPWDD User ID… - User currently has a User ID with a different agency/agency ID. Do NOT enter User ID. Go to part 2. Name Change - User needs to change last name ONLY. No other requests can be made at that time. Go to part 2.
Reactivate Access - 6 months or more since last login (user id account cannot be closed). Go directly to section 3.
Close OPWDD User ID - User no longer employed with agency/no longer need to use User ID account. Go directly to section 4.
*If user requesting more than one account/more than one application, only ONE form should have "I do not have an OPWDD User ID" selected.
Part 2 - Select ONE option from the Application Access Request (grant, modify role OR revoke).
Grant - User needs to gain access to a specific application. Go to part 3.
Modify Role - User needs to change their current role in CHOICES; the user MUST notate their User ID. Go to part 3. Revoke - User still with agency, needs to remove ONE application from User ID account. CLOSE cannot be chosen. Go to part 3.
Part 3 - Select ONE application from the second drop down menu
Select application needed. External Provisioning staff cannot provide the application needed nor a description of the applications.
Double check all information in section 1 and 2, correct issues, if necessary then print the form.
Section 3 - Statement of Use.
User should double check all information in section 1 and 2 if they did not complete those sections. User needs to read, sign and date.
If “Close OPWDD User ID” OR “Revoke” is chosen, Do NOT make any notation/marks/notes in section 3. Do nothing in section 3.
Section 4 - Executive Approval.
Obtain the Executive Director or AUTHORIZED designee listed with OPWDD signature, printed name and date section 4. Submit the completed form to the appropriate unit listed at the bottom of the form; do not submit this page.
Do NOT submit to the wrong unit or multiple units.
Section 5 - Secure NYS OPWDD Application Authorizer Approval
 OPWDD Agency ID:
OPWDD Agency ID: Select ONE option from drop down menu
Select ONE option from drop down menu