NEW YORK STATE
OFFICE OF ALCOHOLISM AND SUBSTANCE ABUSE SERVICES
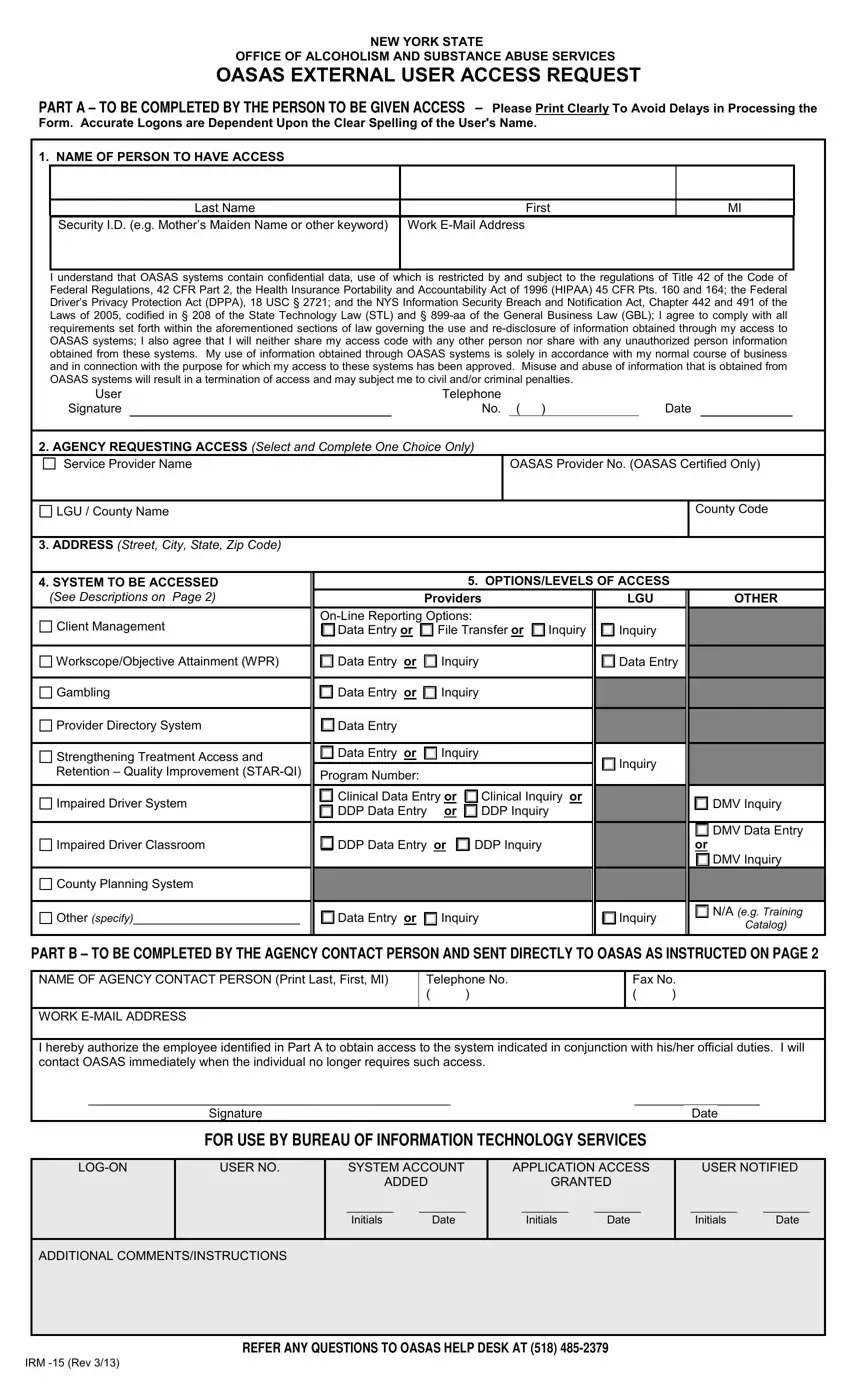
OASAS EXTERNAL USER ACCESS REQUEST
PART A – TO BE COMPLETED BY THE PERSON TO BE GIVEN ACCESS – Please Print Clearly To Avoid Delays in Processing the
Form. Accurate Logons are Dependent Upon the Clear Spelling of the User's Name.
1. NAME OF PERSON TO HAVE ACCESS
Last Name |
First |
Security I.D. (e.g. Mother’s Maiden Name or other keyword) |
Work E-Mail Address |
|
|
I understand that OASAS systems contain confidential data, use of which is restricted by and subject to the regulations of Title 42 of the Code of Federal Regulations, 42 CFR Part 2, the Health Insurance Portability and Accountability Act of 1996 (HIPAA) 45 CFR Pts. 160 and 164; the Federal Driver’s Privacy Protection Act (DPPA), 18 USC § 2721; and the NYS Information Security Breach and Notification Act, Chapter 442 and 491 of the Laws of 2005, codified in § 208 of the State Technology Law (STL) and § 899-aa of the General Business Law (GBL); I agree to comply with all requirements set forth within the aforementioned sections of law governing the use and re-disclosure of information obtained through my access to OASAS systems; I also agree that I will neither share my access code with any other person nor share with any unauthorized person information obtained from these systems. My use of information obtained through OASAS systems is solely in accordance with my normal course of business and in connection with the purpose for which my access to these systems has been approved. Misuse and abuse of information that is obtained from OASAS systems will result in a termination of access and may subject me to civil and/or criminal penalties.
User |
|
Telephone |
|
|
|
Signature |
|
No. |
( |
) |
Date |
2.AGENCY REQUESTING ACCESS (Select and Complete One Choice Only)
OASAS Provider No. (OASAS Certified Only)
LGU / County Name
3.ADDRESS (Street, City, State, Zip Code)
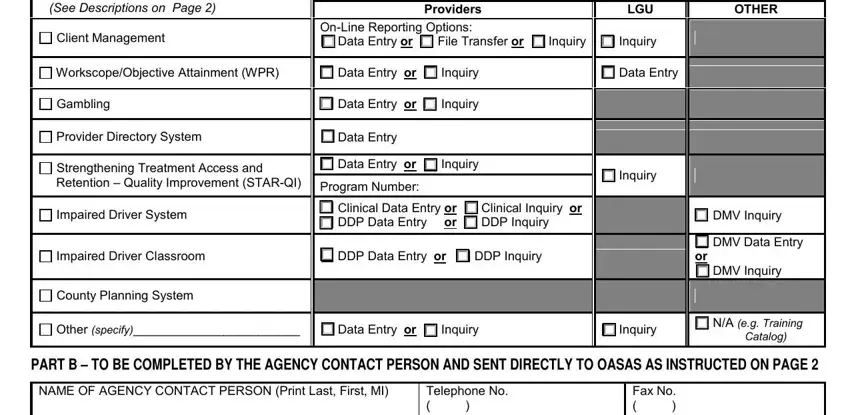
4. SYSTEM TO BE ACCESSED (See Descriptions on Page 2)
Client Management
Workscope/Objective Attainment (WPR)
Gambling
Provider Directory System
Strengthening Treatment Access and Retention – Quality Improvement (STAR-QI)
Impaired Driver System
Impaired Driver Classroom
County Planning System
Other (specify)________________________
5. OPTIONS/LEVELS OF ACCESS
|
Providers |
|
|
LGU |
OTHER |
On-Line Reporting Options: |
|
|
|
|
|
Data Entry or |
File Transfer or |
Inquiry |
Inquiry |
|
Data Entry |
or |
Inquiry |
|
|
Data Entry |
|
Data Entry |
or |
Inquiry |
|
|
|
|
Data Entry |
|
|
|
|
|
|
|
Data Entry |
or |
Inquiry |
|
|
Inquiry |
|
Program Number: |
|
|
|
|
|
|
|
|
|
|
|
Clinical Data Entry or |
Clinical Inquiry |
or |
|
DMV Inquiry |
DDP Data Entry |
or |
DDP Inquiry |
|
|
|
|
|
|
|
|
|
|
|
|
DMV Data Entry |
DDP Data Entry or |
DDP Inquiry |
|
|
|
or |
|
|
|
|
|
|
|
DMV Inquiry |
Data Entry |
or |
Inquiry |
|
|
Inquiry |
N/A (e.g. Training |
|
|
Catalog) |
|
|
|
|
|
|
|
PART B – TO BE COMPLETED BY THE AGENCY CONTACT PERSON AND SENT DIRECTLY TO OASAS AS INSTRUCTED ON PAGE 2
|
NAME OF AGENCY CONTACT PERSON (Print Last, First, MI) |
Telephone No. |
Fax No. |
|
|
( |
) |
( |
) |
|
|
|
|
|
|
WORK E-MAIL ADDRESS
I hereby authorize the employee identified in Part A to obtain access to the system indicated in conjunction with his/her official duties. I will contact OASAS immediately when the individual no longer requires such access.
____________________________________________________ |
|
_______ |
|
______ |
|
|
|
|
Signature |
|
|
|
|
|
|
Date |
|
|
|
|
FOR USE BY BUREAU OF INFORMATION TECHNOLOGY SERVICES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LOG-ON |
USER NO. |
|
SYSTEM ACCOUNT |
APPLICATION ACCESS |
|
USER NOTIFIED |
|
|
|
|
|
ADDED |
GRANTED |
|
|
|
|
|
|
|
|
|
________ |
________ |
________ |
________ |
|
________ |
________ |
|
|
|
|
|
Initials |
Date |
Initials |
Date |
|
Initials |
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDITIONAL COMMENTS/INSTRUCTIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REFER ANY QUESTIONS TO OASAS HELP DESK AT (518) 485-2379 |
|
|
|
IRM -15 (Rev 3/13) |
|
|
|
|
|
|
|
|
|
|
INFORMATION AND INSTRUCTIONS
PURPOSE
The purpose of this form is to provide a means for agencies (services providers, Local Governmental Units [LGUs] and other authorized agencies) to arrange for their staff to obtain access to a variety of on-line data systems maintained by OASAS in order to process data associated with these systems electronically.
PROCESSING THE ACCESS REQUESTS
Step 1 - The person for which access is being requested completes Part A (Sections 1-4), including the security ID (his/her mother’s maiden name or other keyword) which will be used for security purposes, and identifying information by which they can be contacted (telephone number, fax number and e-mail address).
Department of Motor Vehicles employees who work at county DMV office locations indicate county office in the LGU / County Name, e.g. DMV Albany County. All other DMV employees enter DMV Central Office in the Service Provider Name.
The systems to be accessed (described below) should be selected, including the appropriate processing option under which data will be processed and the appropriate level of access, consistent with the tasks to be performed.
The individual signs the form agreeing that he/she will abide by the system’s users requirements.
Step 2 - The agency contact person reviews the information completed in Part A verifying that the appropriate access is being requested and completes Part B authorizing such access and providing identifying information by which they can be contacted (telephone number and email address) and mails the form directly to:
NYS OASAS
1450 Western Avenue
Albany, NY, 12203-3526
Attention: HELP DESK
or faxes the form to:
(518) 457-2387 – Attention: HELP DESK
(please do not fax information & instruction pages)
OASAS will contact the individual directly to provide a confidential access code and instructions on establishing an individual password.
DESCRIPTIONS OF SYSTEMS TO BE ACCESSED
Client Management System - enables providers of treatment services to report client demographic and service delivery data on- line. This includes data on admissions, discharges, transfers, service delivery data, including units of service, and waiting list data. The system can accept inquiries and generate operational and statistical reports. The system is accessible by service providers and associated LGU administrators.
Workscope/Objective Attainment System - enables providers of funded treatment services to view quarterly performance data and related reports based on Workscope mandatory objective performance targets identified for various performance indices for their programs.
Gambling System – enables providers of gambling treatment services to report demographic and service delivery data on-line. This includes data on admissions, discharges, service delivery data, including units of service and waiting list data. The system can accept inquiries and generate operational and statistical reports. The system is accessible by service providers and associated LGU administrators.
Provider Directory System – enables providers (treatment, prevention, LGU) to maintain their contact information and limited information regarding their provider and programs.
Strengthening Treatment Access and Retention – Quality Improvement (STAR–QI) – helps treatment providers become more efficient in processing their clients by tracking key indicators from the first request for service through the first month of treatment. STAR-QI is a combination of the Strengthening Treatment Access and Retention – State Infrastructure (STAR – SI) and Network for Improving Addiction Treatment (NIATx) initiatives.
Impaired Driver System – enables providers of clinical services to impaired driving offenders and Drinking Driver Program (DDP) services to report client service delivery information on-line for motorists arrested for or convicted of impaired driving related offenses pursuant to section 1192 of the Vehicle and Traffic Law. Data collected via this system will be shared with the Department of Motor Vehicles (DMV) as required for their relicensing process.
Impaired Driver Classroom – enables county DMV employees to enroll eligible motorists in New York State DDPs. Approved NYS DDPs will access the system to view rosters online, transfer or reschedule motorists to other classes as necessary, and enter information regarding instructors and class locations. Central Office DMV employees will access the system for the purpose of identifying approved DDP locations and instructors.
County Planning System – is a Web-based application that was developed as a cost-effective and efficient means for completing and submitting required annual planning forms, communicating with the field on planning-related matters, and providing timelier and more accessible data resources.
SECURITY FEATURES
To assist the user in managing their password, the assignment of a “hint” is provided. The use of the “hint” allows the user to assign a new password if they have forgotten their current one. This “self management” feature is available via the Change Password link on the OASAS Applications login page.
If an incorrect login or password is used to access an OASAS system, the account will be disabled after five consecutive attempts. Access rights will only be restored by contacting the OASAS Help Desk. Please note the login and password are case sensitive.
If a user does not access an OASAS system during a consecutive 90 day period, the account will be disabled. Access rights will only be restored by contacting the OASAS Help Desk.
If a user does not access an OASAS system during a consecutive 400 day period, the account will be closed and access rights terminated. Access rights will only be restored by resubmitting a new IRM-15 request.
IRM -15 (Rev 3/13)