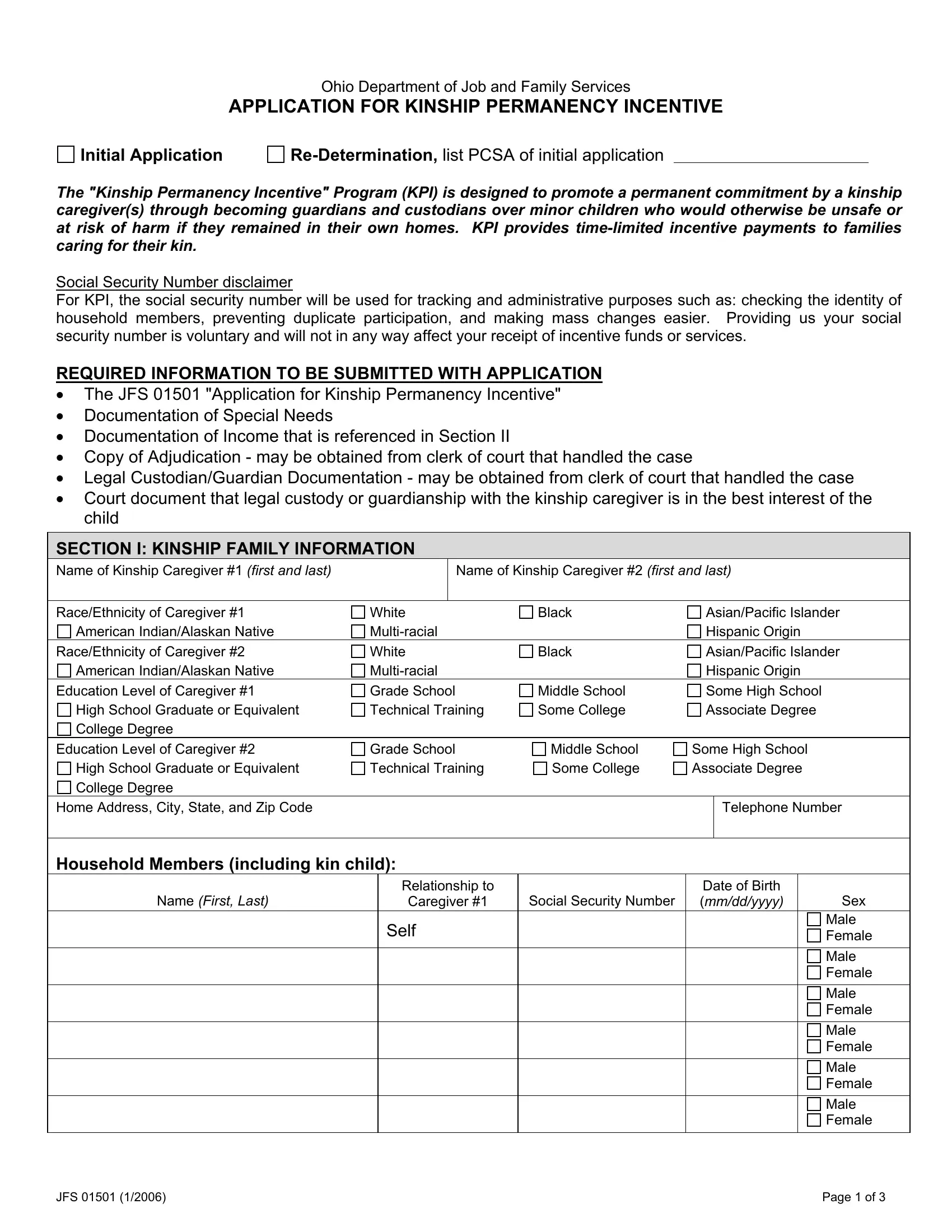
The Ohio Department of Job and Family Services' JFS 01501 form serves a crucial role in the Kinship Permanency Incentive (KPI) Program, offering a systematic avenue for kinship caregivers to apply for or re-determine their eligibility for time-limited incentive payments. This initiative underscores the state's commitment to ensuring children at risk of harm due to unsafe home conditions have the chance to thrive in the care of kinship guardians or custodians. By emphasizing the importance of a secure and permanent home environment, KPI addresses the vital needs of those children whose wellbeing depends on the stability provided by close relatives or family friends willing to take on a nurturing role. The form requires detailed information, including the caregivers' personal and financial details, the child or children's background, and specific legal documentation to corroborate the kinship arrangement's legitimacy and the child's special needs. Caregivers are prompted to provide documentation that supports the application, such as proof of income, legal custody or guardianship papers, and a court's determination regarding the child's living situation, highlighting the program's thorough approach to verifying eligibility and ensuring aid reaches those genuinely in need. Through its meticulous requirements, the JFS 01501 form embodies a gateway to support and stability for kinship families, reflecting the broader objectives of child welfare and family support systems to foster safer, healthier, and more resilient communities.
| Question | Answer |
|---|---|
| Form Name | Form Jfs 01501 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | 01501 kinship incentive program application form |
