Filling out l tmb form is straightforward. We created our tool to really make it convenient to use and assist you to complete any PDF online. Listed below are steps you will want to stick to:
Step 1: Select the button "Get Form Here" on this website and select it.
Step 2: Now you may edit the l tmb form. You can use the multifunctional toolbar to add, erase, and alter the content material of the form.
Fill in the l tmb form PDF by entering the content meant for every single part.
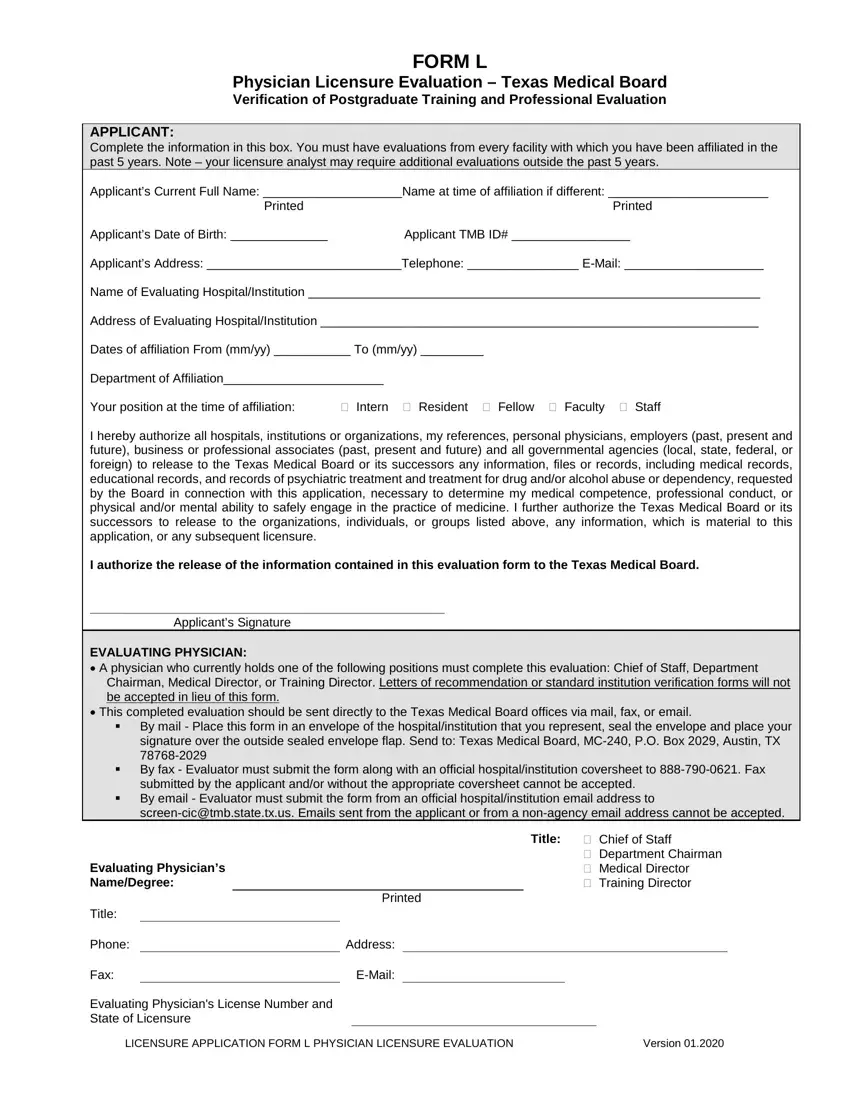
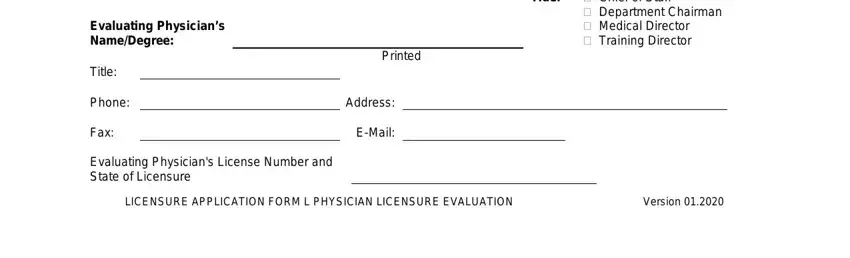
Please insert the information inside the box Title Chief of Staff, Department Chairman Medical, Evaluating Physicians NameDegree, Title, Phone, Fax, Printed, Address, EMail, Evaluating Physicians License, and LICENSURE APPLICATION FORM L.
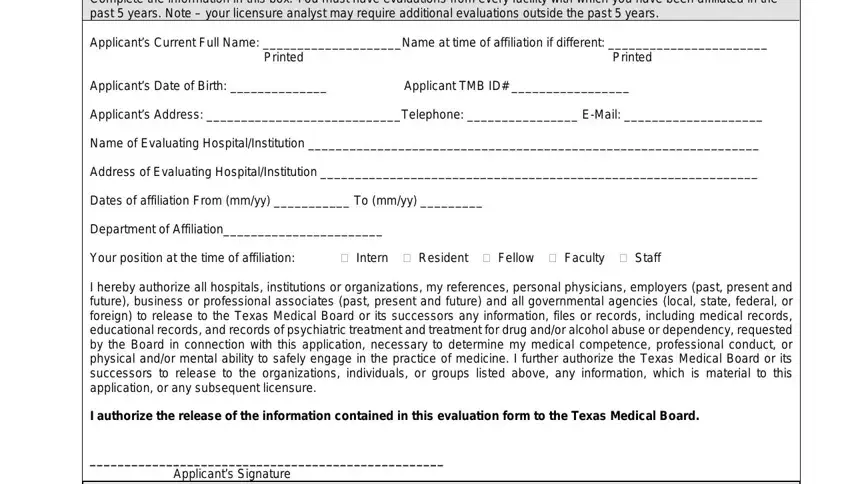
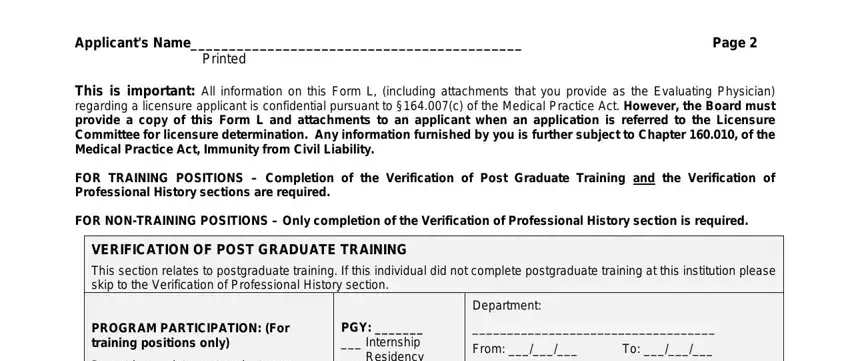
The program will ask you to give certain vital information to instantly fill out the area FORM L, Applicants Name Printed, Page, This is important All information, FOR TRAINING POSITIONS Completion, FOR NONTRAINING POSITIONS Only, VERIFICATION OF POST GRADUATE, PROGRAM PARTICIPATION For training, PGY Internship Residency, Department, and From.
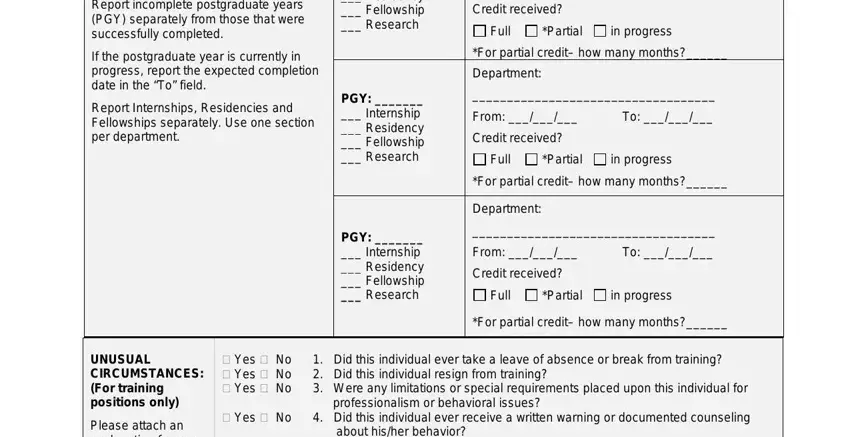
When it comes to paragraph Report incomplete postgraduate, If the postgraduate year is, Report Internships Residencies and, PGY Internship Residency, PGY Internship Residency, Credit received, Full, Partial, in progress, For partial credit how many months, Department, From, Credit received, Full, and Partial, state the rights and obligations.
Terminate by taking a look at the following fields and completing them as required: Applicants Name, Page, VERIFICATION OF PROFESSIONAL, This evaluation is based on, Review of Credential File, How long have you known the, Is the applicant related to you, Do you know the applicant well, Yes, Yes, Has your acquaintance with the, Yes, Do you consider the applicant, a Reliable b Ethical c Of good, and Please rate the applicant.
Step 3: After you click the Done button, your prepared form may be transferred to any kind of your devices or to electronic mail given by you.
Step 4: Prepare duplicates of your template. This may save you from upcoming worries. We cannot read or distribute your information, hence you can be confident it's going to be safe.
